HMPV: INTRODUCTION
Human metapneumovirus (HMPV) is a viral pathogen first identified in 2001, though it is believed to have circulated undetected in human populations for decades prior to its discovery. It is a member of the Paramyxoviridae family, which also includes other well-known respiratory viruses such as respiratory syncytial virus (RSV) and the parainfluenza viruses. HMPV is now recognized worldwide as an important cause of lower respiratory tract diseases in infants, young children, immunocompromised individuals, and the elderly. Despite its relatively recent identification, HMPV has garnered significant attention because of its prevalence, the spectrum of clinical disease it exhibits, and the potential complications it can cause in high-risk groups.
Like other respiratory viruses, HMPV spreads primarily through respiratory droplets and close contact, commonly resulting in illnesses that range from mild upper respiratory tract infections to more severe presentations such as pneumonia and bronchiolitis. Over the past two decades, research into HMPV has expanded significantly, providing insights into its virology, pathogenesis, and epidemiology. This chapter aims to present a comprehensive overview of HMPV, covering its history, classification, virological structure, modes of transmission, biological behavior, clinical manifestations, diagnosis, management, prevention, and directions for future research.
HMPV: HISTORY AND DISCOVERY
Human metapneumovirus was first described in 2001 by a Dutch research team led by B. van den Hoogen. Through a systematic analysis of nasopharyngeal samples from pediatric patients suffering from severe respiratory infections, they identified a novel pathogen using a combination of cell culture and molecular techniques. This previously unknown virus was closely related to avian metapneumovirus (AMPV), which causes respiratory diseases in birds. Subsequent analyses of archived biological specimens indicated HMPV had infected humans worldwide for several decades prior to its formal detection.
Although HMPV’s documented history is fairly short, retrospective examinations have confirmed that HMPV infections likely occurred, but remained undiagnosed, as far back as the 1950s. The initial discovery of HMPV filled an important gap in the catalog of respiratory pathogens that cause significant morbidity, particularly in pediatric populations. Researchers deduced that this virus is globally distributed, and prevalence studies showed infections occur in a pattern similar to RSV, an established and closely related respiratory pathogen. The discovery of HMPV has thus underscored the need for ongoing surveillance of respiratory viruses and highlighted how novel pathogens can circulate undetected for many years.
HMPV: TAXONOMY AND CLASSIFICATION
Human metapneumovirus belongs to the Pneumovirinae subfamily within the Paramyxoviridae family. Historically, the Pneumovirus genus included HMPV’s close relative, RSV; subsequently, HMPV was placed within its own genus called Metapneumovirus, reflecting its close relationship to avian metapneumovirus. Genetic studies have revealed that HMPV can be divided into two main genetic lineages, A and B, which can be further subdivided into at least two sublineages each (A1, A2, B1, and B2). These different genetic groups sometimes manifest differing antigenic properties, although cross-protective immune responses appear to exist to some degree.
The classification of HMPV is based largely on sequence analysis of the fusion (F) and attachment (G) glycoproteins—key proteins on the viral surface that play important roles in host cell interactions and immune recognition. While antigenic differences among the lineages and sublineages can be detected, clinical disease associated with each variant appears generally similar. Nonetheless, analyzing genetic diversity is crucial for understanding the virus’s evolutionary patterns, epidemiological distribution, and for designing effective vaccines and diagnostic tools.
HMPV: VIRAL STRUCTURE AND GENOME
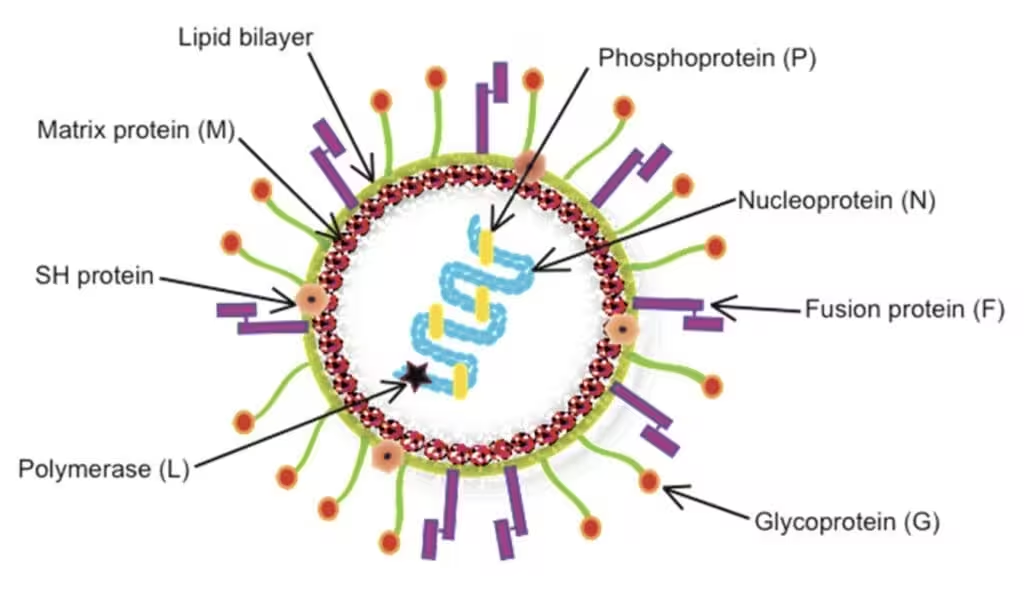
HMPV is an enveloped, negative-sense, single-stranded RNA virus that measures approximately 150–600 nm in length, with a typical paramyxovirus pleomorphic shape. Like other members of the Paramyxoviridae family, it forms filamentous particles and can appear spherical or elongated. The envelope is derived from the host cell membrane during viral budding, and embedded in this envelope are the two major surface glycoproteins: the attachment (G) glycoprotein and the fusion (F) glycoprotein.
The HMPV genome is roughly 13 kilobases long and encodes at least eight open reading frames. These genes include the nucleoprotein (N), phosphoprotein (P), matrix protein (M), fusion protein (F), matrix protein 2 (M2), small hydrophobic protein (SH), glycoprotein (G), and the large polymerase (L). Among these, the F and G proteins are primarily involved in viral entry and host immune system interactions. The F protein is essential for membrane fusion, facilitating viral entry into host cells by merging the viral envelope with the host cell membrane. The G protein mediates initial viral attachment to host cells, though it is less conserved than F and tends to show more genetic variability.
HMPV: EPIDEMIOLOGY
Since its identification, HMPV has been shown to circulate worldwide, exhibiting seasonal patterns in temperate regions that often resemble those of RSV and influenza, typically peaking in winter and early spring. However, seasonality can vary by geographic location, with tropical regions seeing year-round activity that may peak during rainy seasons. The virus predominantly affects young children—particularly those younger than five—and is a leading cause of bronchiolitis and pneumonia in this age group.
Studies have demonstrated that most children acquire HMPV infection by the age of five, indicating a high prevalence of exposure in early childhood. Reinfections commonly occur throughout life, though typically in older children and adults, the symptoms remain less severe. However, in specific high-risk populations—such as the elderly and persons with compromised immune systems—HMPV can cause severe lower respiratory tract complications, often necessitating hospitalization. Outbreaks in long-term care facilities and hospital wards are not uncommon and have prompted measures for infection control and containment.
HMPV: TRANSMISSION AND PATHOGENESIS
Transmission of HMPV occurs primarily through respiratory droplets generated when an infected person coughs or sneezes. Close contact and fomites, such as contaminated surfaces or objects, can also facilitate person-to-person spread. The virus typically enters through the upper respiratory tract, binding to epithelial cells via the G glycoprotein. Upon attachment, the F glycoprotein mediates fusion of the viral and cellular membranes, allowing the viral genome to enter the cytoplasm and initiate replication.
Following entry, HMPV undergoes replication in the cell’s cytoplasm, generating new viral proteins and genomes. Viral assembly occurs at the plasma membrane, and newly formed virions then bud out, incorporating host cell membrane components. The immune response during HMPV infection involves both innate and adaptive components. In the innate response, interferons (IFNs) and cytokines are released early, while natural killer (NK) cells and macrophages target infected cells. During the adaptive response, virus-specific T cells and neutralizing antibodies develop, reducing viral load. However, the virus can cause immune and epithelial cell damage, contributing to inflammation and symptomatic disease, particularly in the lower airways. This inflammation can manifest as bronchiolitis, pneumonia, or exacerbations of asthma and chronic obstructive pulmonary disease (COPD) in susceptible individuals.
HMPV: IMMUNE RESPONSE
Upon infection with HMPV, the innate immune system acts as the first line of defense. Pattern recognition receptors (PRRs), such as Toll-like receptors (TLRs) and retinoic acid-inducible gene I (RIG-I)-like receptors, detect viral components and trigger the release of cytokines. Interferons, particularly type I (IFN-α/β), play a critical role in curbing viral replication by activating antiviral pathways in neighboring cells. NK cells also contribute to this early control by directly lysing infected cells.
Meanwhile, the adaptive immune response involves B cells producing virus-specific antibodies and T cells (CD4+ helper and CD8+ cytotoxic T lymphocytes) targeting infected cells. Neutralizing antibodies directed against the F glycoprotein are especially important in controlling viral infection and preventing reinfection. However, reinfections are common; while individuals usually experience milder symptoms upon re-encounter with HMPV, complete immunity is not typically established. This partial immunity could be due to the virus’s genetic variability, particularly in the G protein, or due to waning immunity over time, exemplifying a viral strategy that allows continued circulation within the human population.
HMPV: CLINICAL MANIFESTATIONS
HMPV infections span a clinical spectrum that ranges from asymptomatic or mild upper respiratory illness to severe lower respiratory tract disease. In otherwise healthy children, manifestations may include runny nose, nasal congestion, sore throat, cough, fever, and wheezing. When the infection progresses to the lower airways, it can cause bronchiolitis or pneumonia. Bronchiolitis, characterized by inflammation of the small airways, is most frequently seen in infants and toddlers and may present with difficulty breathing, wheezing, and heightened respiratory effort.
In older children and adults, HMPV typically results in mild cold-like symptoms, though more severe disease can occur in individuals with underlying chronic conditions such as asthma or heart disease. In immunocompromised patients, whether due to HIV infection, solid organ or hematopoietic stem cell transplantation, or immunosuppressive therapies, HMPV can precipitate significant morbidity characterized by prolonged viral shedding, severe pneumonia, and sometimes death. In the elderly, infection can manifest as COPD exacerbations or pneumonia and lead to significant healthcare utilization. Notably, differentiating HMPV infections from those caused by other respiratory pathogens solely by clinical manifestations can be challenging, as overlap in clinical features is extensive.
HMPV: LABORATORY DIAGNOSIS
Definitive diagnosis of HMPV infection requires laboratory testing, because the clinical signs and symptoms are not specific enough to distinguish it from other respiratory viruses. Common diagnostic modalities include:
• Molecular methods: Reverse transcription-polymerase chain reaction (RT-PCR) assays are considered the gold standard for HMPV detection. These tests identify viral RNA in respiratory specimens (nasopharyngeal or oropharyngeal swabs, washes, or aspirates) with high sensitivity and specificity. Real-time RT-PCR is increasingly used in clinical laboratories.
• Antigen detection: Immunofluorescence assays can be used to detect HMPV antigens in respiratory samples with moderate sensitivity. These tests are faster than molecular methods but may be less sensitive.
• Viral culture: Although HMPV can be propagated in certain cell lines (e.g., LLC-MK2 cells), isolation in cell culture is time-consuming and not routinely performed in most clinical laboratories. Culture-based techniques are more often reserved for research purposes.
• Serology: Serologic assays to detect a rise in antibody titers between acute and convalescent sera can be used in retrospective analyses or for epidemiological purposes. However, in acute clinical settings, serologic testing is less commonly employed because of its limited utility in guiding immediate patient management.
HMPV: TREATMENT AND MANAGEMENT
At present, the mainstay of HMPV management is supportive care. For mild infections, this may include hydration, antipyretics for fever control, and nasal saline spray or humidification to relieve nasal congestion. In more severe cases, particularly in pediatric or high-risk populations, hospitalization may be necessary for supplemental oxygen, intravenous fluids, and close respiratory monitoring. In severe bronchiolitis or pneumonia, advanced supportive measures—such as high-flow nasal cannula, noninvasive ventilation, or mechanical ventilation—may be required if respiratory failure develops.
Ribavirin, an antiviral agent used for RSV in some high-risk patients, has been evaluated experimentally for HMPV with inconsistent results, and it is not routinely recommended. Research into novel antiviral drugs targeting HMPV is ongoing, though none have yet been licensed for widespread clinical use. The role of immunomodulators (e.g., corticosteroids) remains unclear and is typically reserved for specific situations, such as asthma exacerbations triggered by HMPV. Passive immunotherapy with monoclonal antibodies directed against HMPV’s F protein (similar to palivizumab for RSV) is an area of interest; however, as of now, there is no clinically approved monoclonal antibody prophylaxis or therapy for HMPV. Therefore, current management strategies rely heavily on providing adequate supportive care and vigilant clinical monitoring.
HMPV: PREVENTION AND CONTROL
Preventing HMPV transmission poses similar challenges to preventing the spread of other common respiratory pathogens. Frequent hand hygiene, avoiding close contact with infected individuals, and adherence to respiratory etiquette (covering coughs and sneezes, wearing masks in clinical settings) can reduce transmission in households and healthcare facilities. Environmental disinfection of surfaces and objects that may be contaminated with respiratory secretions is also effective in limiting the spread of HMPV.
Outbreaks of HMPV in hospitals and nursing homes highlight the importance of infection control measures. Implementing isolation precautions for known or suspected HMPV-infected patients and using personal protective equipment (PPE) such as gloves, gowns, and masks can significantly reduce healthcare-associated transmission. Proactive surveillance in healthcare settings can detect outbreaks early, allowing targeted interventions to mitigate further spread.
Vaccine development has been hampered by several factors, including the virus’s genetic variability and challenges posed by the immune response. While substantial research has focused on the F protein as a potential vaccine candidate—owing to its critical role in viral entry—no HMPV vaccine has reached clinical use. Technological advances in reverse genetics systems are providing new opportunities for constructing live-attenuated or subunit vaccine candidates. Nonetheless, it may be some time before a safe, effective, and widely available HMPV vaccine is realized.
HMPV: SPECIAL POPULATIONS AND COMPLICATIONS
Although young children represent the most visibly affected population, HMPV can be particularly concerning in elderly individuals and the immunocompromised. In long-term care facilities, outbreaks can occur, occasionally sparking a wave of hospitalizations due to pneumonia. The risk of exacerbations of underlying pulmonary or cardiac conditions also rises with HMPV infection, contributing to morbidity and mortality in older adults.
Immunocompromised persons, including hematopoietic stem cell and solid organ transplant recipients, may present with more prolonged and severe courses of illness. Their compromised immune system can delay virus clearance, leading to lung injury and progression to respiratory failure. Some studies have reported that donor-derived HMPV infections can occur in the context of transplanted organs, demonstrating the potential for unique transmission pathways in these populations. In both pediatric and adult patients with cancer, HMPV can cause severe respiratory disease during times of neutropenia or high immunosuppression, highlighting the importance of vigilant surveillance and preventive measures.
Another special group includes individuals with chronic respiratory diseases such as asthma or COPD. For them, HMPV acts as a potent trigger for exacerbations, similar to how other viruses like RSV and influenza inflame the airways. Patients may experience significant wheezing, shortness of breath, and a decline in pulmonary function, potentially requiring aggressive respiratory support and, in severe cases, hospitalization. Understanding these complications underscores the importance of targeted prevention strategies and early detection in high-risk populations.
FUTURE DIRECTIONS
Research into HMPV is continuously evolving, fueled by the recognition that it is a common and sometimes severe agent of respiratory disease in a broad range of populations. Future directions in HMPV research can be acknowledged in several areas:
• Vaccine Development: Scientists are leveraging new vaccine platforms—such as mRNA, viral vectors, and subunit-based technologies—to develop promising HMPV vaccine candidates. As we learn more about the antigenic properties of the F and G proteins, strategies that elicit strong, durable immune responses may emerge, improving prospects for an effective vaccine.
• Antiviral Therapies: While supportive care remains the mainstay of HMPV treatment, there is a pressing need for direct-acting antivirals or monoclonal antibody therapies that could reduce hospitalizations and severe disease in vulnerable populations. Novel inhibitors targeting the viral polymerase or specific glycoproteins are under investigation.
• Improved Diagnostics: Advances in multiplex molecular panels have accelerated diagnosis of respiratory viruses, including HMPV. Continued refinement in point-of-care testing will allow clinicians to make more rapid, accurate diagnoses in real time, guiding appropriate clinical management and infection control measures.
• Pathogenesis and Immunity: There is still much to unravel about the viral-host interactions that dictate disease severity and immune protection. Elucidating how HMPV modulates host immunity and understanding the key elements of protective immunity remains essential to developing next-generation therapies and vaccines.
CONCLUSION
Though discovered relatively recently, human metapneumovirus is undoubtedly a significant respiratory pathogen with a global impact. It infects all ages, but it remains a particularly important cause of disease in young children, the elderly, and immunocompromised individuals. Its seasonality, overlapping clinical features with other viruses, and capacity for severe lower respiratory tract infection demand that healthcare providers and public health experts regard HMPV with the same vigilance they apply to established respiratory pathogens like RSV and influenza.
The absence of a licensed vaccine or targeted antiviral underscores the continued burden of this virus, along with the economic toll associated with hospitalizations, outpatient visits, and complications. Research efforts aimed at elucidating the molecular mechanisms behind HMPV replication and pathogen–host interactions are crucial for informing efforts to develop safe and efficacious vaccines and treatments. In the meantime, standard infection control practices and supportive management remain the most effective strategies to combat HMPV infections, underscoring the universal value of general hygiene measures, early diagnosis, and concerted public health efforts.
As scientific understanding of HMPV expands, it is likely that novel diagnostic approaches, therapeutics, and prophylactic measures will be developed. The story of HMPV is emblematic of the evolving nature of virology and epidemiology: despite humankind’s long history with respiratory pathogens, novel viruses can still emerge—or be recognized for the first time—shaping future directions and informing preparedness strategies for respiratory infections. The case of HMPV thus provides both a cautionary tale about the constantly changing landscape of infectious diseases and a reminder of the potential strides modern science can make in addressing them.
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.
Community Notes
Join the Discussion
Ask follow-up questions, add clinical perspective, or share a useful clarification for the next reader.