

Introduction
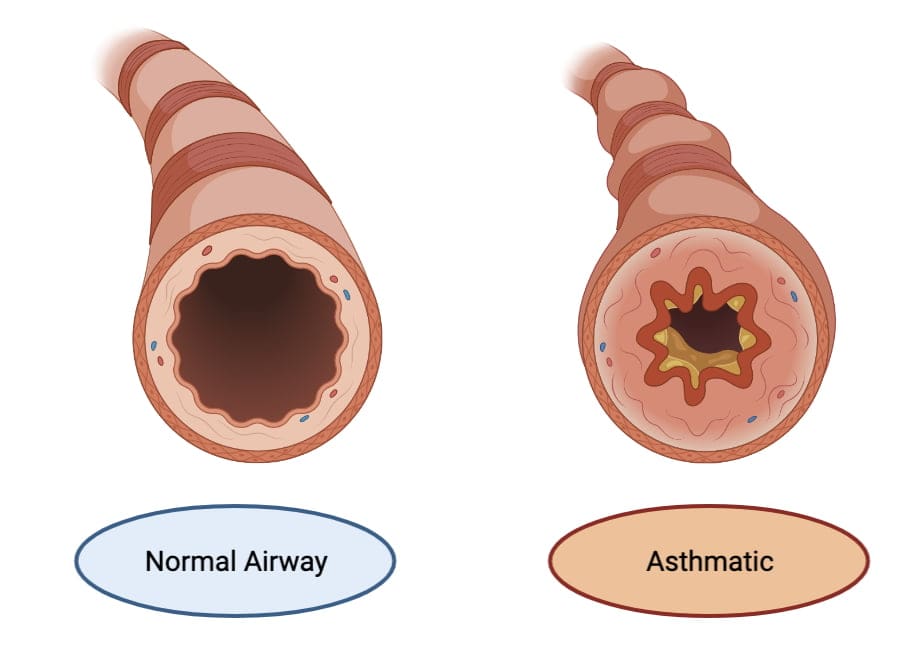
Asthma is a chronic inflammatory disease of the airways, characterized by bronchial hyperresponsiveness, variable airflow obstruction, and repeated episodes of wheezing, coughing, chest tightness, and dyspnea. This condition affects more than 300 million people worldwide, imposing a significant burden on healthcare systems, impacting economic productivity, and compromising quality of life (Goodman & Gilman, 2018). While the etiology of asthma includes a complex interplay of genetic predispositions and environmental factors (e.g., allergens, pollutants, infections), the hallmark pathophysiology is rooted in airway inflammation and reversible bronchoconstriction.
Over the past several decades, significant advances in our understanding of airway inflammation have reshaped the pharmacotherapeutic approaches to asthma. Where once bronchodilators were the mainstay of disease management, contemporary guidelines emphasize the vital role of anti-inflammatory therapies and stepwise escalation or de-escalation according to symptom control (Katzung, 2020). In modern practice, a multidimensional plan that includes reliever (rescue) medications, controller (maintenance) strategies, trigger avoidance, and close monitoring of lung function is pursued to minimize airway remodeling and reduce acute exacerbations.
This comprehensive review explores the pharmacotherapy of asthma, presenting the key agents, their mechanistic underpinnings, and how they fit into clinical guidelines. By tying these interventions to the underlying immunopathology of the disease, we underscore how individualized therapy can optimize outcomes and reduce the burdens associated with this prevalent chronic respiratory disorder (Rang & Dale, 2019).
Pathophysiology of Asthma: A Pharmacological Rationale
At the core of asthma lies a heightened inflammatory response in the airways, driven by various cells and mediators. T-helper 2 (Th2) lymphocytes, eosinophils, mast cells, and neutrophils (in some phenotypes) collectively release cytokines—such as interleukin (IL)-4, IL-5, IL-13—that perpetuate inflammation, mucus hypersecretion, and airway hyperresponsiveness. The airway smooth muscle constricts in response to direct or indirect stimuli (e.g., allergens, irritants), leading to airflow obstruction and the characteristic symptoms of asthma (Goodman & Gilman, 2018).
Contemporary medications target different arms of this inflammatory cascade, reduce bronchial hyperresponsiveness, or relax the bronchial smooth muscle. Understanding these pathways justifies the use of inhaled corticosteroids (ICS), long-acting β2 agonists (LABAs), leukotriene modulators, and novel biologic therapies. The personalized selection of pharmacotherapy depends on disease severity, frequency of exacerbations, spirometric patterns, and phenotypic considerations (Katzung, 2020).
Quick-Relief (Reliever) Medications: Short-Acting Bronchodilators
Short-Acting β2-Adrenergic Agonists (SABAs)
Short-acting β2 agonists like albuterol (salbutamol) and levalbuterol are the gold-standard reliever agents. These drugs bind β2 receptors on bronchial smooth muscle, triggering adenylyl cyclase to increase cyclic AMP levels, resulting in smooth muscle relaxation and rapid bronchodilation.
- Onset and Duration: SABAs usually start working within 5 minutes and last approximately 3–6 hours.
- Clinical Applications: Indicated for acute relief of bronchospasm during asthma attacks, prevention of exercise-induced bronchoconstriction, and as-needed use in milder forms of asthma (Rang & Dale, 2019).
- Adverse Effects: Potential side effects include tachycardia, tremor, palpitations, and hypokalemia (in overdose situations or frequent use). Excessive reliance on SABAs signals poor disease control.
Short-Acting Anticholinergics (SAMAs)
Although more commonly favored in chronic obstructive pulmonary disease (COPD), ipratropium bromide can provide additional bronchodilation in acute asthma exacerbations. It blocks muscarinic (M3) receptors in the lungs, reducing vagal tone and inhibiting bronchoconstriction. It is most often combined with a SABA in acute severe exacerbations (Katzung, 2020).
Controller Medications: Inhaled Corticosteroids (ICS)
Mechanism of Action
Inhaled corticosteroids rank as the cornerstone of asthma prophylaxis. By binding glucocorticoid receptors in airway cells, ICS reduce the transcription of pro-inflammatory cytokines (e.g., IL-4, IL-5) and upregulate anti-inflammatory proteins. The net effect is a dampening of airway inflammation, decreased hyperresponsiveness, and reduced frequency of exacerbations (Goodman & Gilman, 2018).
Common ICS Agents
- Budesonide
- Fluticasone propionate
- Beclomethasone dipropionate
- Ciclesonide
- Mometasone furoate
Clinical Benefits and Usage
Long-term ICS therapy substantially lowers the risk of severe exacerbations and hospital visits. ICS are started in patients whose asthma symptoms occur more than twice weekly or when there is any feature of persistent disease. Doses should be titrated to the lowest effective level that maintains good control (Rang & Dale, 2019).

Adverse Effects
Systemic effects of inhaled steroids are minimized compared to oral steroids, but local side effects can include oral thrush (candidiasis), dysphonia, and mild throat irritation. Rinsing the mouth and spacer devices help reduce these complications.
Long-Acting β2-Adrenergic Agonists (LABAs)
Mechanism and Role
When added to inhaled corticosteroids, long-acting β2 agonists provide sustained bronchodilation—spanning typically 12 hours. They act via the same cyclic AMP pathway as SABAs, but with extended action due to their lipophilicity and receptor kinetics (Katzung, 2020).
Representative LABAs
- Salmeterol
- Formoterol
- Vilanterol (often paired with fluticasone in combination inhalers)
Clinical Application
LABAs are never used as monotherapy in asthma, as they do not address underlying inflammation and can mask poorly controlled disease if used alone. Instead, combining a LABA with ICS (e.g., fluticasone/salmeterol, budenoside/formoterol) markedly improves symptom control and reduces exacerbations, especially in moderate to severe persistent asthma (Rang & Dale, 2019).
Adverse Effects
Similar to SABAs: tremor, tachycardia, potential for hypokalemia in rare situations. However, these adverse effects tend to be less frequent at standard inhaled doses.
Long-Acting Muscarinic Antagonists (LAMAs)
Mechanism of Action
Although anticholinergic drugs are mainstays in COPD management, they increasingly find use in asthma, especially in patients whose disease remains poorly controlled on ICS/LABA combinations (Goodman & Gilman, 2018). Tiotropium and umeclidinium block M3 receptors in the airways, inhibiting acetylcholine-mediated bronchoconstriction for over 24 hours.
Place in Therapy
Adding tiotropium to ICS ± LABAs may modestly improve lung function and reduce exacerbations in moderate to severe asthma. This strategy suits patients with frequent nighttime symptoms or those who remain symptomatic despite standard combination therapies (Katzung, 2020).
Side Effects
Generally well tolerated, but anticholinergic effects such as dry mouth, urinary retention, and pharyngeal irritation can occasionally occur.
Leukotriene Pathway Modifiers
Rationale
Leukotrienes such as LTC4, LTD4, and LTE4 are potent mediators in asthma that promote bronchoconstriction, mucus secretion, and airway hyperresponsiveness. Targeting this pathway can be particularly beneficial in allergic or exercise-induced asthma (Rang & Dale, 2019).
Classes and Key Agents
- Leukotriene Receptor Antagonists (LTRAs): Montelukast, Zafirlukast. These block the CysLT1 receptor, reducing bronchoconstriction and inflammation.
- 5-Lipoxygenase Inhibitors: Zileuton prevents leukotriene synthesis itself, curbing production of LTB4 and cysteinyl leukotrienes (Katzung, 2020).
Clinical Uses
- Mild persistent asthma as add-on to low-dose ICS.
- Aspirin-exacerbated respiratory disease, given that leukotriene pathways can be amplified in aspirin-sensitive asthma.
- Pediatric patients or those who prefer oral therapies.
Adverse Effects
While generally safe, montelukast has possible neuropsychiatric effects (e.g., agitation, mood changes), and zileuton can affect liver enzymes, demanding periodic monitoring (Goodman & Gilman, 2018).
Methylxanthines (Theophylline)
Pharmacologic Action
Theophylline, a methylxanthine derivative, exerts bronchodilatory and mild anti-inflammatory activity, possibly by inhibiting phosphodiesterase enzymes (thereby increasing cAMP) and blocking adenosine receptors. Historically a mainstay, it has been superseded by inhaled agents with better safety profiles (Rang & Dale, 2019).
Therapeutic Considerations
- Narrow Therapeutic Index: Serum levels typically aimed between 5–15 μg/mL. Levels >20 μg/mL increase risk of arrhythmias, seizures, nausea, and other toxicities.
- Drug Interactions: Metabolized by the CYP1A2 and CYP3A4 pathways, meaning interactions with inducers (e.g., rifampin) or inhibitors (e.g., cimetidine) can drastically alter levels (Katzung, 2020).
Given these concerns, theophylline is rarely used in routine asthma, reserved primarily for special situations or resource-limited settings.
Systemic Corticosteroids
High-Level Role
Despite robust anti-inflammatory activity, oral or intravenous corticosteroids (e.g., prednisone, methylprednisolone) are typically reserved for acute severe exacerbations or for short “burst” courses in moderate exacerbations to regain control (Goodman & Gilman, 2018). Chronic oral steroid therapy is discouraged because of significant side effects—hypercortisolism, osteoporosis, weight gain, hyperglycemia, adrenal suppression, and psychological changes.
Indications
- Acute Asthma Attacks: Oral/IV steroids help quell airway inflammation, typically continued for 5–10 days.
- Severe Persistent Asthma: In patients who remain uncontrolled with maximal inhaled therapies, low-dose oral steroids may be used, though with caution (Rang & Dale, 2019).
Biologic Therapies for Severe Asthma
Background
A segment of severe asthmatic patients remains symptomatic despite optimal high-dose ICS + LABA ± LAMA. Many of these individuals exhibit eosinophilic or allergic phenotypes, driven by IgE or IL-5–mediated pathways. Biologics targeting these pathways can transform disease control (Katzung, 2020).
Anti-IgE Therapy: Omalizumab
- Mechanism: Binds circulating IgE, preventing it from attaching to mast cells and basophils. Reduces allergic inflammation and frequency of exacerbations.
- Indication: Moderate to severe allergic asthma with elevated serum IgE not controlled on standard combination therapy.
- Administration: Subcutaneous every 2–4 weeks.
- Side Effects: Injection site reactions, rare anaphylaxis (Goodman & Gilman, 2018).
Anti-IL-5 / Anti-IL-5R Agents: Mepolizumab, Reslizumab, Benralizumab
- Mechanism: By inhibiting IL-5 signaling or depleting eosinophils, they reduce eosinophilic inflammation.
- Indications: Eosinophilic phenotype with recurrent exacerbations, high peripheral eosinophil counts.
- Administration: Typically subcutaneous or IV every 4–8 weeks.
IL-4/IL-13 Pathway Inhibitors: Dupilumab
- Mechanism: Dupilumab blocks the IL-4 receptor α subunit, inhibiting both IL-4 and IL-13 signaling crucial to Th2-driven airway inflammation.
- Indication: Moderate to severe type 2 (T2) high asthma with elevated biomarkers (eosinophils, fractional exhaled nitric oxide).
- Benefits: Reduced exacerbations, improved lung function, decreased dependence on oral steroids (Katzung, 2020).
Considerations for Biologics
These advanced therapies carry a high cost, requiring specialist assessment and adherence to strict criteria. They are safe and often dramatically improve disease control in the right population. Monitoring includes tracking eosinophil levels, allergic markers, and frequency of exacerbations (Rang & Dale, 2019).
Common Combination Inhalers
ICS/LABA Formulations
- Fluticasone/Salmeterol
- Budesonide/Formoterol
- Mometasone/Formoterol
- Fluticasone/Vilanterol
These combination inhalers are central to moderate or severe persistent asthma, often once or twice daily. They combine the anti-inflammatory benefits of an ICS with the bronchodilatory support of a LABA (Goodman & Gilman, 2018).
Triple Therapy (ICS + LABA + LAMA)
Emerging data supports triple-therapy inhalers (e.g., fluticasone furoate/umeclidinium/vilanterol) in severe or frequent exacerbators. Although historically more common in COPD, some patients with severe refractory asthma may derive benefit from a single combined device (Katzung, 2020).
Stepwise Approach to Asthma Management
Global Initiative for Asthma (GINA) Recommendations
Contemporary guidelines emphasize a stepwise approach tailored to symptom control and exacerbation risk:
- Step 1: As-needed low-dose ICS-formoterol or SABA (depending on guidelines).
- Step 2: Low-dose ICS daily + as-needed SABA or as-needed low-dose ICS-formoterol.
- Step 3: Low-dose ICS/LABA plus as-needed SABA or ICS-formoterol.
- Step 4: Medium-dose ICS/LABA ± add-on LAMA. Consider specialist referral.
- Step 5: Refer for phenotyping. Possible biologics (e.g., omalizumab, mepolizumab), high-dose ICS/LABA, or triple therapy (Rang & Dale, 2019).
Frequent re-evaluation ensures therapy is stepped up if control is inadequate, or stepped down to minimize medication side effects when control is maintained (Katzung, 2020).
Managing Acute Asthma Exacerbations
Mild to Moderate Exacerbations
- High-dose SABA (e.g., multiple puffs via MDI or nebulized albuterol)
- Early initiation of oral steroids (e.g., prednisone 40–60 mg for 5–7 days)
- Oxygen supplementation if hypoxemic (Goodman & Gilman, 2018).
Severe, Life-Threatening Attacks
- High-flow oxygen, repeated or continuous nebulized SABA, plus ipratropium bromide
- Systemic corticosteroids (IV or oral)
- IV magnesium sulfate for bronchodilation in resistant cases
- Intubation and mechanical ventilation if respiratory failure ensues (Rang & Dale, 2019)
Measuring peak expiratory flow (PEF) or FEV1 helps track response. Failure to respond or a deteriorating picture demands intensive care.
Special Considerations
Pediatric Patients
- ICS remain first-line. Montelukast is an alternative in mild persistent disease.
- Spacer devices and face masks for inhalers ensure better delivery.
- High caution with biologics, typically reserved for older children with severe uncontrolled asthma (Katzung, 2020).
Pregnancy
- Most ICS (e.g., budesonide) have a good safety record, as do short-acting β2 agonists.
- Maintaining asthma control is paramount, as maternal hypoxia can harm fetal oxygenation. Oral steroid bursts are permissible when needed (Goodman & Gilman, 2018).
Exercise-Induced Bronchoconstriction
- Short-acting β2 agonist inhalation 15 minutes prior to exercise remains a standard prophylactic approach.
- Leukotriene receptor antagonist or ICS/LABA can also reduce exercise-induced symptoms in more persistent cases (Rang & Dale, 2019).
Monitoring and Adherence
Peak Flow Monitoring
Many patients with moderate to severe or poorly controlled asthma benefit from peak expiratory flow self-measurements at home. Peak flow meters allow detection of early declines, prompting timely adjustments in medications.
Medication Adherence
Non-adherence to daily controller therapy is a major barrier to achieving good control. Inhaler technique errors are also rampant, reinforcing the value of repeated education and demonstration. Spacer or valved holding chambers can improve drug delivery from metered-dose inhalers (Katzung, 2020).
Comorbidities
Conditions like rhinosinusitis, GERD, obesity, and sleep apnea can worsen asthma control if unmanaged. Addressing triggers (e.g., allergens, occupational exposures) is also essential to reduce medication burden and limit exacerbations (Goodman & Gilman, 2018).
Evolving Therapies and Future Directions
Novel Biologic Targets
Ongoing research focuses on upstream cytokines and pathways. Agents targeting TSLP (thymic stromal lymphopoietin) or IL-33—key epithelial cytokines—may further refine therapy for type 2–high asthma. For non–type 2 or neutrophilic asthma, other interventions, such as macrolides or tyrosine kinase inhibitors, are under exploration (Rang & Dale, 2019).
Smart Inhalers and Digital Health
Integration of electronic monitoring for inhaler use, adherence apps, and remote telemedicine support is reimagining asthma management in real-time, enabling tailored interventions based on usage patterns and physiologic signals (Katzung, 2020).
Proactive Approaches and Prevention
Immunomodulation in early childhood, allergen immunotherapy, or interventions that modulate the microbiome represent future preventive strategies. These may reshape disease trajectories and reduce reliance on chronic pharmacotherapy (Goodman & Gilman, 2018).
Conclusion
The pharmacotherapy of asthma has evolved into a highly tailored, stepwise approach, merging bronchodilators and anti-inflammatory strategies to control symptoms, prevent exacerbations, and minimize airway remodeling. For the majority of patients, inhaled corticosteroids remain central, complemented by additional long-acting β2 agonists, long-acting muscarinic antagonists, or leukotriene receptor antagonists if needed. In patients with severe, refractory disease—especially those exhibiting specific inflammatory phenotypes—biologic agents targeting IgE, IL-5, or IL-4/13 have revolutionized therapy, substantially reducing exacerbations and steroid use (Rang & Dale, 2019).
Ongoing innovations in drug delivery, expansion of biological treatments, and a deeper understanding of asthma phenotypes continue to advance the field. Emphasis on patient education, inhaler technique, and adherence remains crucial. By tailoring interventions to individual disease characteristics and systematically monitoring outcomes with peak flow or spirometry, clinicians can optimize control, ensuring that people with asthma lead active, healthy lives with minimal limitations (Katzung, 2020).
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition.
- Katzung BG, Basic & Clinical Pharmacology, 14th Edition.
- Rang HP, Dale MM, Rang & Dale’s Pharmacology, 8th Edition.
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.