
Introduction
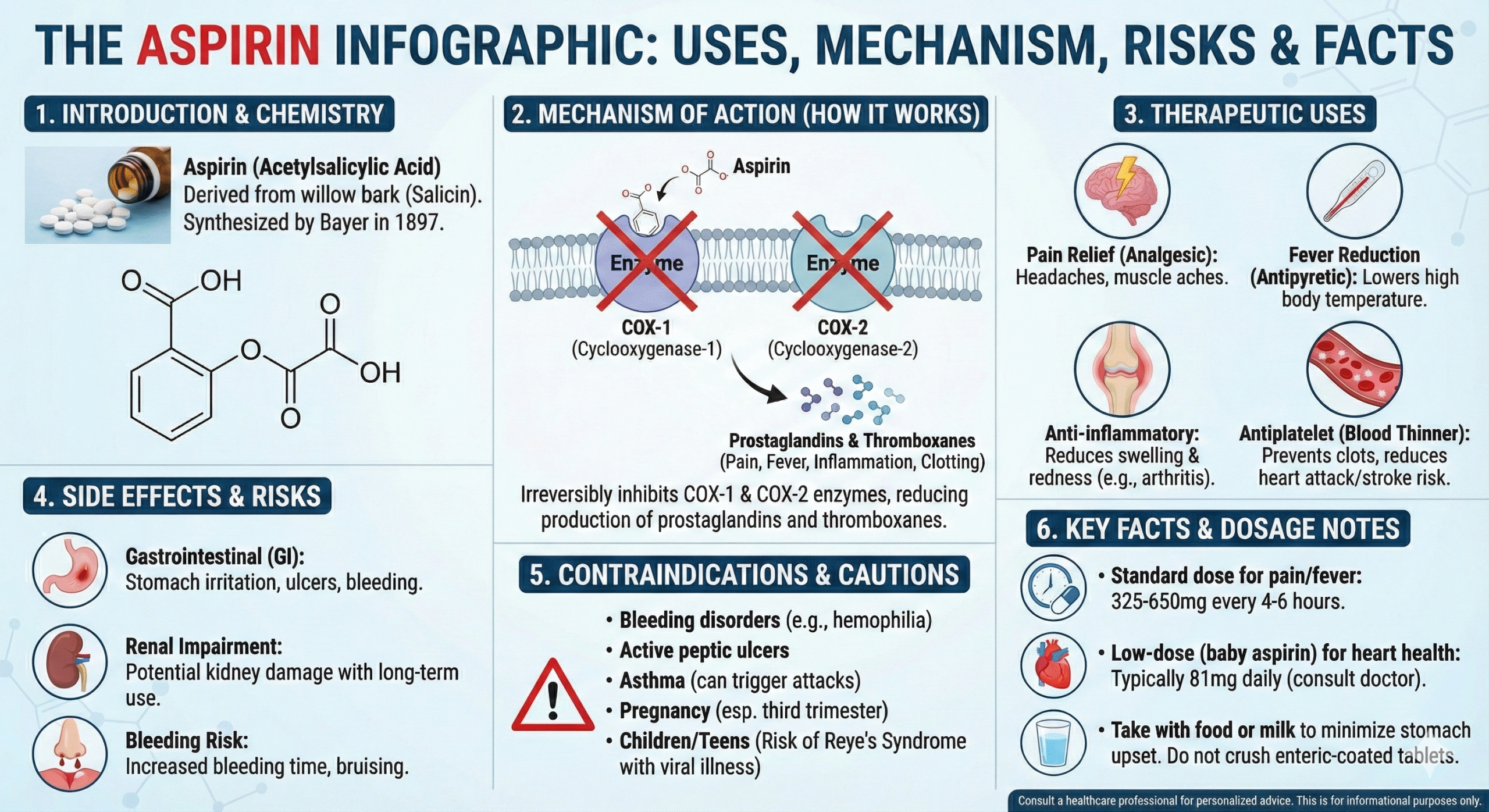
Aspirin—chemically known as acetylsalicylic acid—is among the most widely used medications across the globe. Renowned for its analgesic, antipyretic, anti-inflammatory, and, at low doses, antithrombotic actions, aspirin’s versatility has made it a mainstay in clinical practice for well over a century. Discovered in the late 19th century, aspirin’s enduring role owes to its capacity to provide effective pain relief, reduce fever, mitigate inflammatory states, and protect against cardiovascular events. Moreover, growing evidence suggests additional benefits in colorectal cancer prophylaxis for selected populations (Katzung, 2020).
This comprehensive review explores the pharmacology of aspirin, underscoring how it exerts its multifaceted actions and how clinicians optimize its use across a spectrum of indications. Leveraging well-established resources, including “Goodman & Gilman’s The Pharmacological Basis of Therapeutics,” “Katzung’s Basic & Clinical Pharmacology,” and “Rang & Dale’s Pharmacology,” we discuss into aspirin’s chemical properties, mechanisms of action, pharmacokinetics, clinical applications, adverse effects, and evolving considerations. Through understanding aspirin’s complexities, medical professionals can continue to harness its benefits while mitigating potential harms.
Chemistry and Historical Perspectives
Chemical Structure
Aspirin (acetylsalicylic acid) is the acetylated derivative of salicylic acid. An ester linkage integrates the acetyl group with the phenolic hydroxyl of salicylic acid, conferring aspirin’s unique capacity to irreversibly inhibit certain enzymes. This structural modification to the salicylate backbone underpins aspirin’s characteristic acetylating property (Goodman & Gilman, 2018).
Historical Discovery
- Origins in Willow Bark: Salicin, discovered in willow bark, was recognized for antipyretic and analgesic actions centuries ago.
- 19th Century Synthesis: In 1897, scientists at Bayer successfully synthesized stable acetylsalicylic acid, branding it “Aspirin.”
- Rapid Adoption: By 1900, aspirin’s use spread globally as an over-the-counter remedy for pain and fever, eventually evolving into prescription contexts for cardiovascular prophylaxis (Rang & Dale, 2019).
Mechanism of Action
Cyclooxygenase Inhibition
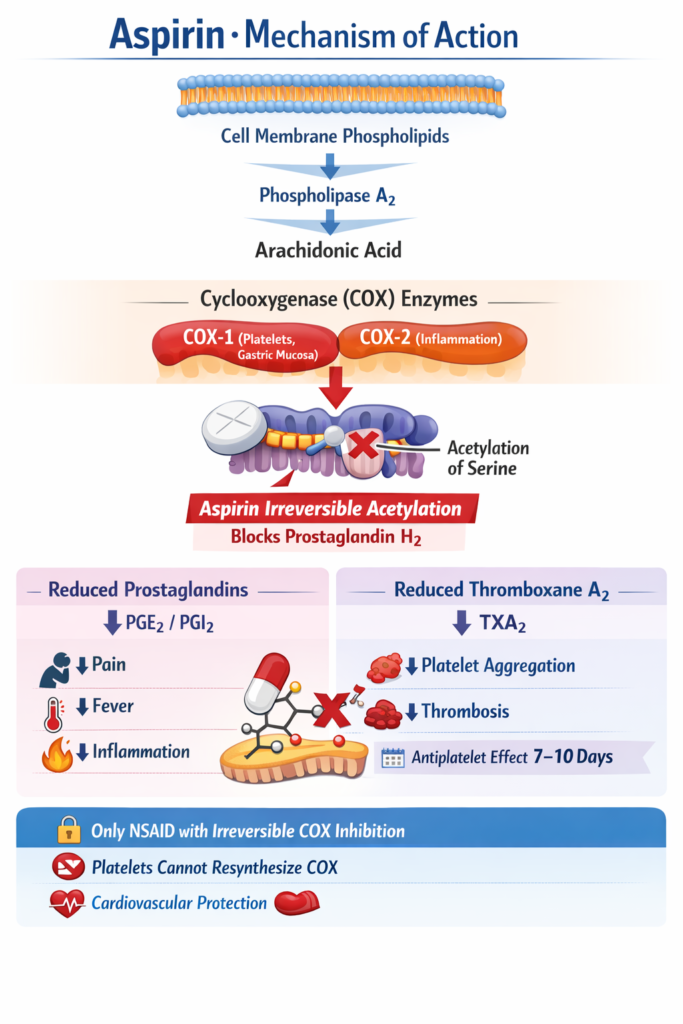
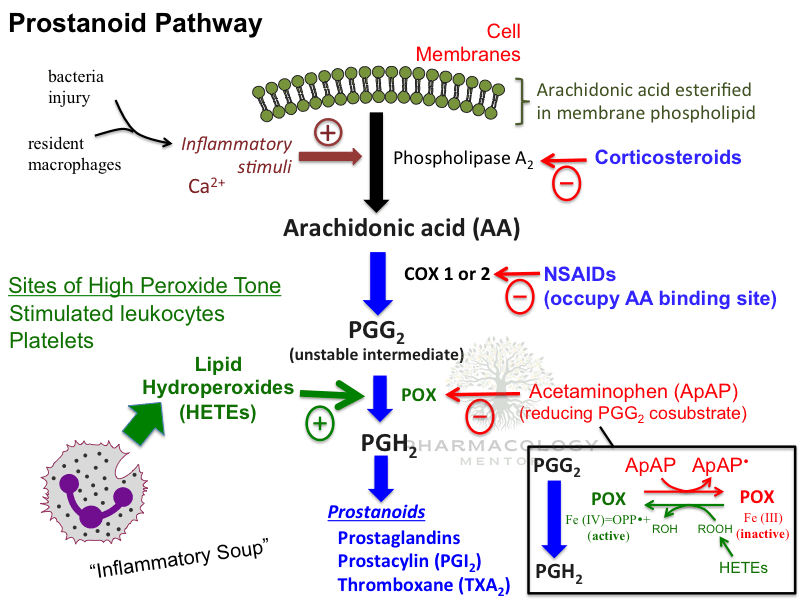
Aspirin’s hallmark property is irreversible inactivation of cyclooxygenase (COX) enzymes—namely COX-1 and COX-2—through acetylation of a key serine residue within their active sites. Subsequent to this, the enzyme is unable to convert arachidonic acid into prostaglandins and thromboxanes (Katzung, 2020).
- COX-1: Constitutive enzyme involved in the synthesis of prostaglandins crucial for gastroprotective mucus, renal function, and platelet function (thromboxane A2 synthesis).
- COX-2: Inducible enzyme upregulated in inflammatory states, generating prostaglandins linked to inflammation, pain, and fever (Goodman & Gilman, 2018).
By irreversibly blocking COX-1, aspirin reduces platelet thromboxane A2 (TXA2) production, impairing platelet aggregation for the lifespan of the platelet (~7–10 days). This effect underlies aspirin’s antithrombotic benefit at low doses.
At higher doses, aspirin’s inhibition of COX-2 leads to diminished production of pro-inflammatory prostanoids (e.g., prostaglandin E2), accounting for analgesic and anti-inflammatory outcomes (Rang & Dale, 2019).
Additional Mechanisms
- Platelet Effects: Lower doses (75–100 mg/day) selectively reduce TXA2 relative to endothelial prostacyclin (PGI2), endowing aspirin with an antiplatelet advantage.
- Salicylate-Specific Anti-inflammatory: High doses of salicylates, beyond COX blockade, can influence other pathways such as NF-κB and oxidative stress responses, supplementing anti-inflammatory capacity (Goodman & Gilman, 2018).
Pharmacokinetics
Absorption
- Oral Administration: Rapid GI absorption, particularly in the stomach and upper small intestine.
- pH-Dependent: In acidic environments, nonionized salicylic acid crosses membranes easily. Aspirin’s dissolution is also influenced by dosage forms such as enteric coating (slower onset but potentially reduced GI irritation) (Rang & Dale, 2019).
Distribution
- Protein Binding: At typical therapeutic levels, ~80–90% binds to plasma proteins (mainly albumin). With saturating high doses, protein binding diminishes, raising free salicylate concentrations.
- Tissue Penetration: Aspirin freely crosses placental and blood-brain barriers in sufficiently high concentrations, especially if the plasma pH or protein-binding capacity changes (Katzung, 2020).
Metabolism and Elimination
- Metabolism: Aspirin is rapidly deacetylated to salicylate in serum and tissues. Salicylate is further metabolized in the liver by conjugation (glycine and glucuronide conjugates) and oxidation pathways.
- Zero-Order Kinetics at High Doses: As metabolic pathways become saturated, salicylate elimination follows zero-order kinetics, resulting in prolonged half-life and potential accumulation.
- Urinary Excretion: pH plays a key role: alkalinizing the urine (pH > 7.5) boosts renal clearance of salicylate. Acidic urine retards excretion, favoring toxicity at overdose (Goodman & Gilman, 2018).
Half-Life
- Low Doses: Aspirin’s half-life is ~2–3 hours for the parent compound; salicylate half-life is ~3–12 hours.
- Higher/Overdose: Metabolic saturation leads to much longer half-lives (up to 15–30 hours), raising toxicity risks (Rang & Dale, 2019).
Dose-Dependent Effects and Clinical Uses

Low-Dose Aspirin (75–100 mg daily)
- Antiplatelet Action: Inhibits platelet COX-1, reducing thromboxane A2 formation.
- Clinical Application: Secondary prevention post-myocardial infarction, stroke prophylaxis, stable coronary artery disease, and some primary prevention in high-risk patients.
- Duration: Platelets cannot synthesize new COX, so the effect lasts their lifetime. Daily dosing ensures a continuous pool of non-functional platelets (Katzung, 2020).
Analgesic and Antipyretic (325–650 mg every 4–6 hours)
- Moderate Doses: Aspirin efficiently suppresses prostaglandin E2 in the hypothalamus (lowering fever) and peripheral tissues (reducing pain).
- Clinical Application: Headache, musculoskeletal aches, mild inflammatory pains, fever management.
- Onset: Typically 30–60 minutes for analgesic effect (Goodman & Gilman, 2018).
Anti-Inflammatory (High Doses: 3–6 g/day)
- Higher Concentrations: More pronounced inhibition of COX-2–derived prostaglandins.
- Clinical Application: Historically used in rheumatoid arthritis, osteoarthritis, and other inflammatory arthritides. Modern practice often favors NSAIDs with safer GI profiles or COX-2 selective inhibitors (Rang & Dale, 2019).
Very High Doses (Toxic Range)
- Plasma salicylate levels >40–50 mg/dL risk salicylism (tinnitus, vertigo, decreased hearing). Progression beyond 70–100 mg/dL can produce life-threatening salicylate toxicity—metabolic acidosis, respiratory alkalosis, encephalopathy, etc. (Katzung, 2020).
Clinical Indications
Cardiovascular
- Secondary Prevention of Myocardial Infarction (MI): Aspirin is standard of care to reduce recurrence of MI and lower cardiovascular mortality.
- Stroke/TIA Prophylaxis: After non-cardioembolic ischemic stroke or transient ischemic attack, low-dose aspirin diminishes recurrent stroke risk.
- Acute Coronary Syndromes: Chewable aspirin on presentation is cornerstone therapy, combined with other antiplatelet agents (Goodman & Gilman, 2018).
Pain and Fever
- Headache, Musculoskeletal: Combined with caffeine (e.g., in some OTC analgesics) for tension headaches.
- Fever Reduction: In adults (not recommended in children due to Reye’s syndrome risk).
- Moderate Osteoarthritis or mild inflammatory conditions, though overshadowed by ibuprofen and other NSAIDs in many settings (Rang & Dale, 2019).
Rheumatoid Arthritis and Other Inflammatory Arthritides
Historically, high-dose aspirin was a principal therapy. Now replaced by safer NSAIDs or disease-modifying agents, but it remains an option if well-tolerated and cost is a factor (Katzung, 2020).
Colon Cancer Prophylaxis
Evidence suggests that long-term low-dose aspirin might reduce incidence and mortality from colorectal cancer. Mechanisms include COX-2 inhibition in precancerous lesions. Guidelines support individualized risk-benefit analysis for prophylactic aspirin use in older adults (Goodman & Gilman, 2018).
Adverse Effects
Gastrointestinal
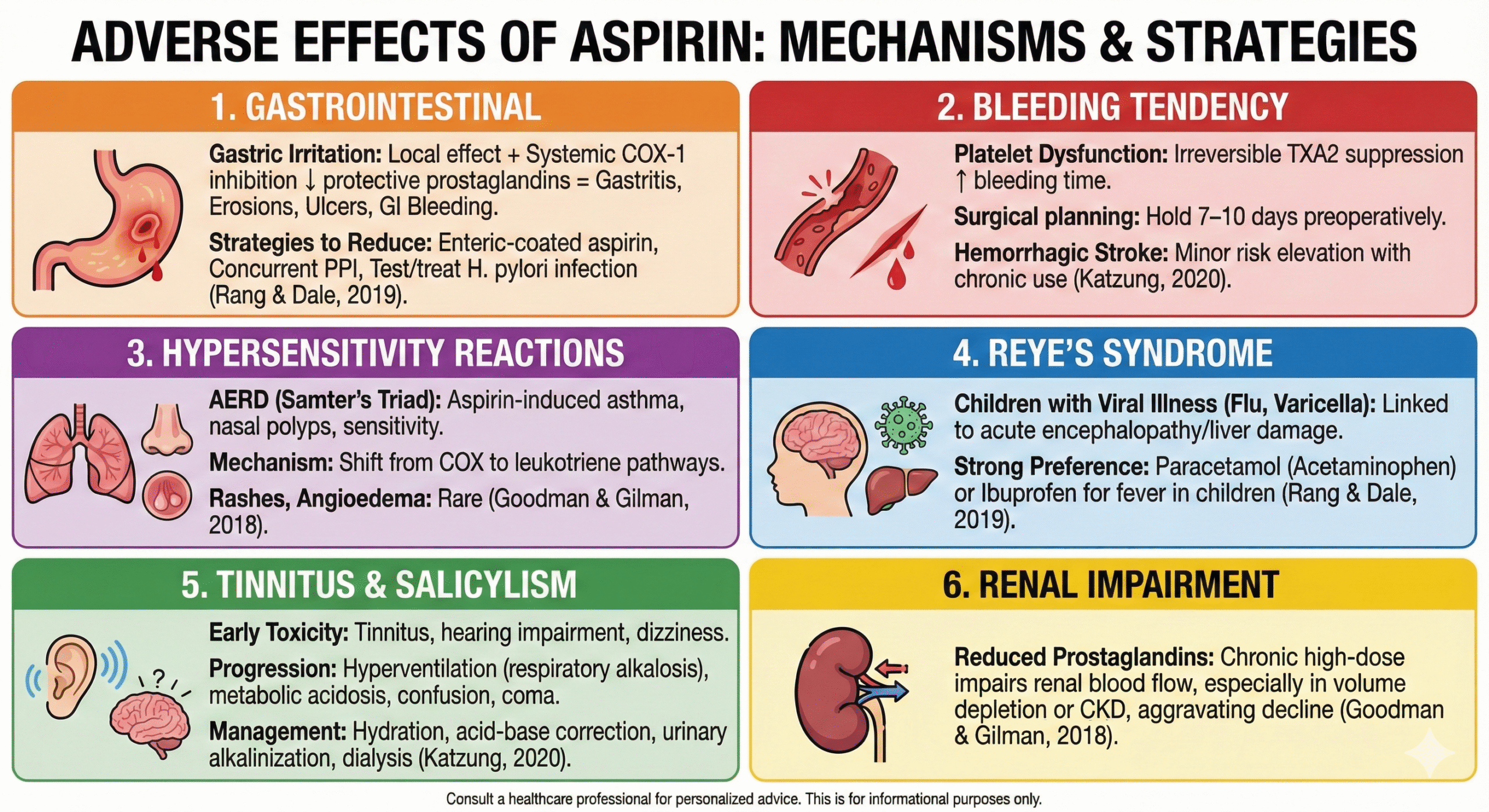
- Gastric Irritation: Local irritant effect plus systemic COX-1 inhibition reduces protective prostaglandins, raising risk of gastritis, erosions, ulcers, and GI bleeding.
- Strategies to Reduce: Enteric-coated aspirin, concurrent proton pump inhibitor (PPI), or testing/treating H. pylori infection can mitigate GI harm (Rang & Dale, 2019).
Bleeding Tendency
- Platelet Dysfunction: Irreversible TXA2 suppression elongates bleeding time. Surgical or procedural planning often requires holding aspirin 7–10 days preoperatively.
- Hemorrhagic Stroke: Minor but notable risk elevation with chronic aspirin usage (Katzung, 2020).
Hypersensitivity Reactions
- Aspirin-Exacerbated Respiratory Disease (AERD): Also known as aspirin-induced asthma or Samter’s triad (nasal polyps, asthma, aspirin sensitivity). Mechanism involves shift from COX to leukotriene pathways.
- Rashes, Angioedema: Rare, but can occur in sensitive individuals (Goodman & Gilman, 2018).
Reye’s Syndrome
- Children with Viral Illness: Aspirin use in pediatrics experiencing influenza or varicella is linked to acute encephalopathy/liver damage. For fever in children, paracetamol (acetaminophen) or ibuprofen is strongly preferred because of the Reye’s risk (Rang & Dale, 2019).
Tinnitus and Salicylism
- Early Sign of Toxicity: Tinnitus, hearing impairment, dizziness.
- Progression: Hyperventilation (respiratory alkalosis), metabolic acidosis, confusion, coma in severe overdose. Adequate hydration, correction of acid-base disturbances, and promoting salicylate excretion (e.g., urinary alkalinization, dialysis) are key in management (Katzung, 2020).
Renal Impairment
- Reduced Prostaglandins: Chronic high-dose aspirin can impair renal blood flow, especially in volume depletion or chronic kidney disease, aggravating kidney function decline (Goodman & Gilman, 2018).
Drug Interactions
NSAIDs
Concomitant use with other NSAIDs can amplify GI injury. Also, if typical NSAIDs (e.g., ibuprofen) are taken around the time of aspirin, they may transiently block aspirin’s access to the COX-1 site in platelets, diminishing its antiplatelet effect. A recommended strategy is to space immediate-release aspirin at least 30 minutes before or 8 hours after NSAIDs (Rang & Dale, 2019).
Anticoagulants and Antiplatelets
Combining aspirin with warfarin, heparin, or novel oral anticoagulants intensifies bleeding risk. Dual antiplatelet therapy with clopidogrel or ticagrelor is standard in certain cardiovascular conditions but meticulously monitored due to augmented bleeding hazards (Katzung, 2020).
Alcohol
Excess alcohol consumption synergistically irritates the gastric lining, elevating the risk of GI bleeding with aspirin usage (Goodman & Gilman, 2018).
Uricosuric Agents (e.g., Probenecid)
Low-dose aspirin can reduce uric acid excretion, negating the effect of uricosuric therapy for gout. Meanwhile, high-dose aspirin might exhibit mild uricosuric activity but is rarely used for managing gout (Rang & Dale, 2019).
Contraindications and Special Populations
Children and Adolescents
Due to Reye’s syndrome risk, avoiding aspirin in individuals <18 years with suspected viral infection is prudent. Alternative antipyretics are advised (Katzung, 2020).
Pregnancy and Lactation
- Third Trimester: Aspirin may prolong gestation, risk premature closure of the ductus arteriosus, and exacerbate bleeding in mother/neonate. Thus, usage is discouraged except for specific low-dose indications (e.g., preeclampsia prophylaxis in high-risk women).
- Breastfeeding: Low-dose aspirin passes minimally into breast milk; high-dose therapy might pose more risk (Goodman & Gilman, 2018).
Peptic Ulcer Disease or History of GI Bleeding
Avoid or strictly regulate aspirin usage if possible; consider PPI co-therapy or alternative agents. Balanced risk assessment is mandatory in patients requiring cardiovascular prophylaxis (Rang & Dale, 2019).
Renal/Hepatic Impairment
Dose adjustments and renal/hepatic function monitoring are recommended at higher aspirin doses to prevent accumulation and toxicity (Katzung, 2020).
Overdose Management
Presentation
Salicylate toxicity can unfold gradually or acutely, characterized by tinnitus, hyperpnea, respiratory alkalosis, metabolic acidosis (particularly in children), dehydration, hyperthermia, and CNS disturbances. In severe cases, respiratory failure, arrhythmias, or coma may occur (Goodman & Gilman, 2018).
Therapeutic Interventions
- Supportive Care: Stabilize airway, breathing, and circulation; correct fluid deficits.
- Activated Charcoal: If ingestion is recent, to limit further absorption.
- Urinary Alkalinization: IV sodium bicarbonate to enhance salicylate ionization and excretion.
- Monitoring Electrolytes and pH: Frequent blood gas measurements; maintain adequate ventilation.
- Hemodialysis: Indicated for severe poisoning (especially with levels >100 mg/dL in acute toxicity or >60 mg/dL in chronic exposure), persistent acidosis, or end-organ compromise (Katzung, 2020).
Emerging and Evolving Concepts
Precision Antiplatelet Therapy
With genetic or phenotypic variance affecting platelet function, ongoing research explores more tailored approaches to aspirin. Platelet function tests or biomarkers might identify individuals who benefit most from daily aspirin or require alternative strategies (Goodman & Gilman, 2018).
Dual and Triple Antithrombotic Therapy
In advanced cardiology, combining low-dose aspirin with P2Y12 inhibitors (e.g., clopidogrel) or with direct oral anticoagulants is used in acute coronary syndrome or stenting. But balancing hemorrhagic complications remains challenging. Trials refine durations and combinations to optimize outcomes (Rang & Dale, 2019).
Cancer Prevention Studies
Large-scale observational data and some randomized trials point to decreased incidence of colorectal and possibly other GI malignancies in chronic aspirin users. Ongoing investigations aim to define optimal dosing, patient selection, and risk–benefit ratios (Katzung, 2020).
Alternative Salicylates and Formulations
Modified release aspirin, intravenous formulations, or novel salicylate derivates attempt to mitigate GI side effects or amplify anti-inflammatory viability. The clinical uptake of these agents, however, remains limited compared to standard aspirin preparations (Goodman & Gilman, 2018).
Clinical Pearls and Best Practices
- Low-Dose Aspirin for CVD Prophylaxis: Indicated for secondary prevention in ischemic heart disease or stroke. Primary prevention requires individual evaluation—risks of GI bleeding must be weighed against atherothrombotic benefits.
- Timing with NSAIDs: Separate administration to preserve aspirin’s irreversible platelet inhibition—take aspirin roughly 30 minutes before ibuprofen or 8 hours after.
- GI Protection: For patients at high GI risk, co-prescribe PPIs or consider using enteric-coated aspirin, though some controversy persists on how effectively it prevents mucosal damage.
- Avoid in Pediatrics with Viral Fevers: The Reye’s syndrome risk significantly outweighs any potential benefit.
- Be Vigilant for Tinnitus: This can be an early sign of salicylate toxicity. Counsel patients to report hearing changes if on moderate or high doses.
- Monitor Renal, Hepatic, and Bleeding: In patients on chronic moderate/high dose therapy, especially older adults or those with comorbid conditions (Rang & Dale, 2019).
Future Directions
- Biomarker-Guided Dosing: Potential for personalized aspirin regimens based on pharmacogenetics or platelet function tests.
- Safer GI Formulations: Ongoing efforts to produce new aspirin derivatives or protective technologies that minimize gastrointestinal side effects.
- Expanded Oncological Roles: Evaluating precise dosing intervals and patient selection for chemo-preventive benefits in diverse malignancies.
- Assessing Combinations: As polypharmacy in cardiac patients grows, new data on the synergy (or conflict) between aspirin and emergent agents (PCSK9 inhibitors, novel antiplatelets) will shape guidelines (Katzung, 2020).
Conclusion
Aspirin (acetylsalicylic acid) endures as a cornerstone medication, lauded for its analgesic, antipyretic, anti-inflammatory, and cardiovascular protective properties. Its mechanism—irreversible COX enzyme blockade—drives not just pain and fever control but also a prolonged antiplatelet effect fundamental to preventing thrombotic events in high-risk patients. Aspirin’s broad dosing range reflects its varied effects: low doses for platelet inhibition, moderate for analgesia/fever, and higher levels for anti-inflammatory efficacy (Goodman & Gilman, 2018).
Nonetheless, clinicians must skillfully balance aspirin’s benefits against common side effects (GI irritation, bleeding) and significant but less frequent issues (Reye’s syndrome, hypersensitivity). Evolving data continue to refine aspirin’s prophylactic roles in primary and secondary cardiovascular disease, colon cancer prevention, and beyond. Future research promises to enhance patient-specific approaches, limiting adverse events while capitalizing on aspirin’s enduring therapeutic strengths (Rang & Dale, 2019).
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition.
- Katzung BG, Basic & Clinical Pharmacology, 14th Edition.
- Rang HP, Dale MM, Rang & Dale’s Pharmacology, 8th Edition.
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.
Community Notes
Join the Discussion
Ask follow-up questions, add clinical perspective, or share a useful clarification for the next reader.