Oral contraceptives (OCs) are hormone-containing medications taken to prevent pregnancy and for management of various gynecologic conditions. They are among the most widely used medicines globally, and have undergone major changes in formulation, pharmacokinetics, and safety since their introduction.
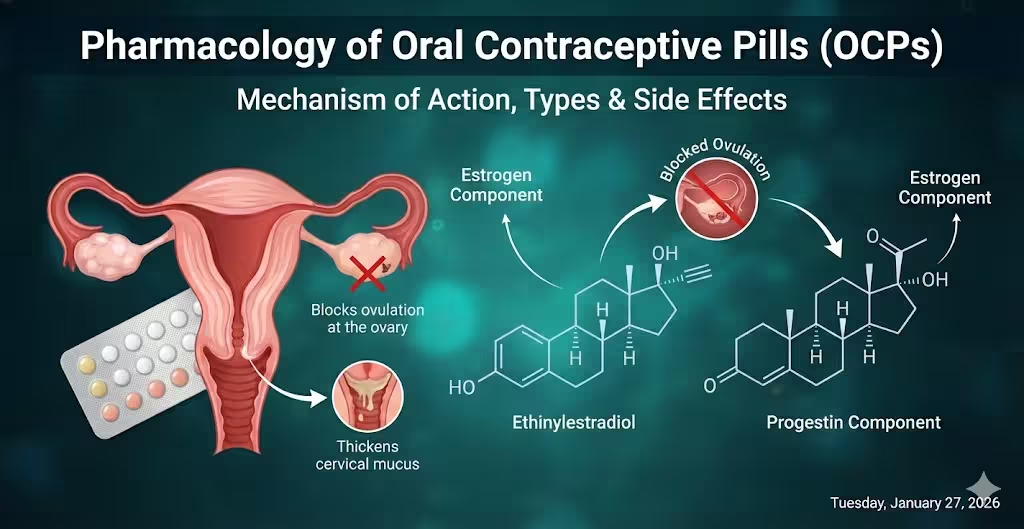
COCs: Suppress ovulation (primary), inhibit development of endometrium (secondary), thicken cervical mucus (secondary). These result from negative feedback of estrogen and progestin on FSH and LH pituitary secretion, prevention of follicle maturation, and mid-cycle LH surge.
POPs: Thicken cervical mucus (primary), alter endometrial environment and suppress ovulation (in up to ~60–70% of cycles for traditional POPs; more reliably in newer POPs).
Pharmacokinetics
Estrogens (ethinylestradiol, estradiol): Well absorbed, significant first-pass hepatic metabolism. Ethinylestradiol is more resistant to breakdown, improving bioavailability (45%). Peak plasma in 1–2 hours, high protein binding (sex hormone binding globulin, albumin), hepatic metabolism (CYP3A4/2C9). t1/2: 12–36 hours.
Progestins: Variable PK per compound. Metabolized by CYP3A4 and others; some have active metabolites (norgestimate → norelgestromin, desogestrel → etonogestrel). t1/2: 8–36 hours.
Steady state: Most OCs reach steady-state within 7 days. Ethinylestradiol rapidly clears; some progestins accumulate more over time. Both undergo enterohepatic circulation, which can be impaired by broad-spectrum antibiotics.
Clinical Indications
Contraception
Menstrual cycle regulation
Treatment of dysmenorrhea, endometriosis, PCOS, acne, hirsutism
Menstrual migraine management
Prevention/treatment of anemia due to heavy menstrual bleeding
Lower risk for ovarian, endometrial, and colorectal cancers with long-term use
Adverse Effects
Effect
Frequency/Type
Management/Notes
Breakthrough bleeding
Common early (esp. low-dose), resolves
Raise estrogen, alternate progestin
Nausea/vomiting
Mild, transient
Take at night
Breast tenderness
Common, dose-dependent
Lower estrogen dose
Mood changes
Mild-moderate, variable
Switch progestin
Decreased libido
Reports vary
No clear solution
Weight gain
Rare with modern pills
Lifestyle
Headache
Switch pill, check for migraine
Avoid if migraine with aura
Hypertension
Up to 4–5% of users; higher in pre-existing cases
Monitor BP
VTE (venous thromboembolism)
RR 1.5–6 (higher risk with EE >35mcg, 3rd/4th gen progestins, obesity, smoking, family risk)
Lowest risk pills preferable, avoid with major risk factors
Stroke/MI
Absolute risk low (<1/100,000 patient-years in <35y), much higher with age, smokers, migraine + aura
Contraindicated if significant risk factors present
Acne
Some progestins worsen, some improve
Consider antiandrogenic pill
Absolute Contraindications
History or risk of VTE, major thrombophilia (Factor V Leiden, SLE/APLS)
Protease inhibitors: may lower or increase OCP levels, depending on PI
Broad-spectrum antibiotics: controversial, only relevant if enterohepatic circulation is interrupted (very rare clinically, except rifampin*)
OCs can alter metabolism of other drugs (warfarin, benzodiazepines, corticosteroids)
Formulations and Regimens
Type/Name
Estrogen Dose
Progestin Type
Cycle Pattern
Monophasic
Fixed EE + fixed progestin for 21 days
Any
21 active + 7 inactive
Biphasic
Fixed EE, increasing progestin
Any
2 dose phases
Triphasic
Increasing EE, progestin, or both
Any
3 dose phases
Extended cycle
EE + progestin 84 days, 7 days inactive
Any
Fewer withdrawal bleeds
POP
No estrogen
Specific
Daily, no hormone-free interval
Clinical Pearls
Modern OCs use <35 mcg EE, lowering estrogen-related risks.
3rd/4th generation progestins (e.g., desogestrel, drospirenone) have reduced androgenic side effects but slightly higher VTE risk.
Continuous/extended cycle pills beneficial for dysmenorrhea, endometriosis, menstrual suppression.
Long-term use lowers risk of ovarian and endometrial cancer; no protective effect for breast cancer.
In obesity or certain drug interactions, less reliable—consider alternate methods.
POPs best for breastfeeding, estrogen contraindications; less forgiving of missed doses.
References
Back DJ, Orme ML. Pharmacokinetic drug interactions with oral contraceptives. Clin Pharmacokinet. 1990;18(6):472–495.
Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th ed. New York: McGraw-Hill; 2017.
Oral Contraceptive Pills—StatPearls [Internet]. 2024 Feb 28.
Wikipedia. Combined Oral Contraceptive Pill.
Choosing a combined oral contraceptive pill. Aust Prescr. 2015;38(1):6–11.
Contraception—StatPearls. 2023 Jul 23.
Osmosis. Oral Contraceptives. Jan 2025.
Xin X, Yuan C, et al. Pharmacokinetics of Oral Combination Contraceptive Drugs Containing Ethinyl Estradiol and Levonorgestrel in Healthy Female Chinese Volunteers. Thieme. 2016.
How to cite this page - Vancouver Style
Mentor, Pharmacology. Oral Contraceptives: OCPs. Pharmacology Mentor. Available from: https://pharmacologymentor.com/oral-contraceptives-ocps/. Accessed on March 11, 2026 at 22:51.
Post Views:98
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.