
Non-steroidal anti-inflammatory drugs (NSAIDs) are cornerstone analgesic, antipyretic, and anti-inflammatory agents whose primary mechanism is inhibition of cyclooxygenase (COX) enzymes to reduce prostaglandin and thromboxane synthesis. A complete pharmacology chapter should cover COX biology, detailed classification, pharmacokinetics/dynamics, therapeutic uses, adverse effects, drug interactions, special populations, and evidence-based risk mitigation strategies from standard pharmacology texts and regulatory advisories.
What NSAIDs are
NSAIDs encompass a heterogeneous group of structurally distinct agents that share analgesic, antipyretic, and anti-inflammatory actions via inhibition of COX-1 and/or COX-2, with aspirin uniquely producing irreversible COX-1 inhibition in platelets. COX-1 is constitutive and supports gastric mucosal protection, renal blood flow, and platelet aggregation, whereas COX-2 is largely inducible in inflammation, so differential selectivity shapes efficacy and toxicity profiles across the class.
COX pathway and mechanism
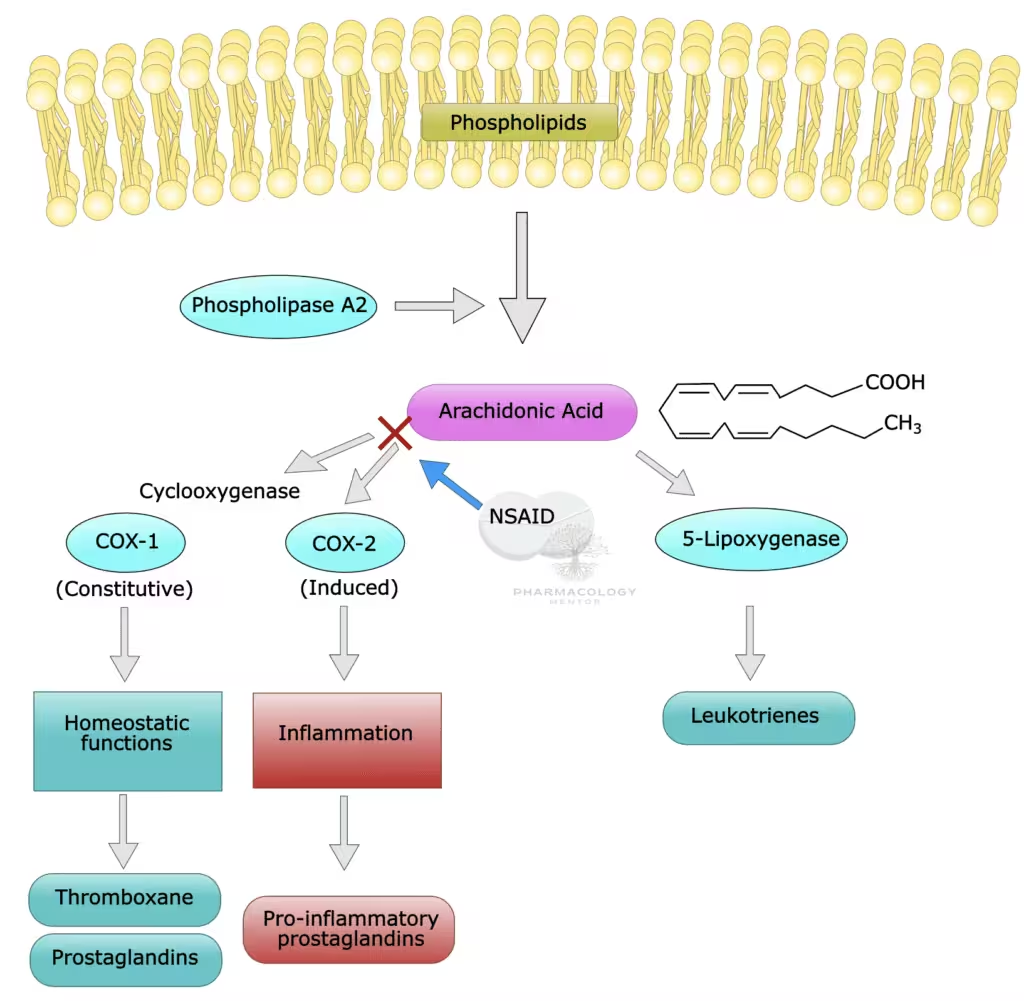
- COX enzymes convert arachidonic acid to prostaglandin H2, the precursor of prostaglandins and thromboxanes that modulate pain, fever, inflammation, vascular tone, and platelet function.
- Nonselective NSAIDs reversibly inhibit both COX-1 and COX-2, while coxibs (e.g., celecoxib) preferentially inhibit COX-2 to preserve gastric COX-1–dependent cytoprotection at comparable anti-inflammatory doses.
- Aspirin acetylates COX irreversibly, giving sustained antiplatelet effects until new platelets are generated, which underlies its use in thrombosis prevention distinct from other NSAIDs.
Core pharmacologic effects
- Analgesia arises from reduced peripheral prostaglandin-mediated nociceptor sensitization and central modulation, lowering inflammatory pain and pain from tissue injury.
- Antipyresis reflects decreased hypothalamic PGE2 synthesis, restoring thermoregulatory set point in fever.
- Anti-inflammatory efficacy stems from reduced vasodilator prostaglandins and vascular permeability mediators at inflamed sites, though NSAIDs do not modify underlying disease drivers in immune arthritides.
Classification of NSAIDs
NSAIDs can be classified by COX selectivity, chemistry, and duration of action, which correlates with clinical use, dosing interval, and adverse effect patterns.
By COX selectivity
- Nonselective COX inhibitors: ibuprofen, naproxen, diclofenac, indomethacin, ketoprofen, ketorolac, piroxicam, meloxicam (preferential COX-2 at low dose), sulindac, oxaprozin, tolmetin, mefenamic acid, nabumetone.
- COX-2 selective (coxibs): celecoxib is widely available; rofecoxib and valdecoxib were withdrawn due to cardiovascular safety concerns.
- Aspirin (acetylsalicylic acid): unique irreversible COX-1 inhibition in platelets with NSAID-class analgesic/antipyretic/anti-inflammatory actions at higher doses.
By chemical class with examples
- Salicylates: aspirin (acetylated), diflunisal, salsalate.
- Propionic acids: ibuprofen, naproxen, ketoprofen, flurbiprofen, fenoprofen, oxaprozin.
- Acetic acids: diclofenac, indomethacin, sulindac, etodolac, ketorolac.
- Enolic acids (oxicams): piroxicam, meloxicam.
- Anthranilic acids (fenamates): mefenamic acid, meclofenamate.
- Naphthylalkanones: nabumetone (prodrug).
- Coxibs: celecoxib (with prior rofecoxib and valdecoxib withdrawn).
By duration (clinically oriented)
- Short/intermediate half-life agents enabling rapid onset and flexible dosing: ibuprofen, diclofenac, ketorolac.
- Longer half-life agents enabling once-daily dosing but accumulating risk with sustained exposure: piroxicam, oxaprozin, naproxen (intermediate-long), meloxicam.
Comparison table (class, selectivity, clinical notes)
Pharmacokinetics (class features)
- Most NSAIDs are well absorbed orally, highly protein bound, variably undergo enterohepatic recycling, and are hepatically metabolized with renal excretion of metabolites, making renal function and hepatic metabolism key determinants of exposure and safety.
- Half-lives vary from hours (ibuprofen, diclofenac) to a day or more (piroxicam, oxaprozin), influencing dosing intervals and steady-state accumulation.
- Topical diclofenac formulations provide effective local delivery for osteoarthritis and soft-tissue injuries with lower systemic exposure and reduced systemic adverse effects compared to oral routes.
Pharmacodynamics nuances
- Analgesia is greatest for inflammatory and somatic pain states, with ceiling effects for simple analgesia beyond which adverse effects predominate; opioid-sparing benefits are recognized in perioperative multimodal regimens.
- Antiplatelet effects: non-aspirin NSAIDs reversibly inhibit platelet COX-1 and can blunt aspirin’s irreversible antiplatelet effect when coadministered in close temporal proximity, which is clinically relevant for secondary prevention.
Therapeutic indications
- Symptomatic relief in osteoarthritis, rheumatoid arthritis, spondyloarthritis, acute gouty arthritis, dysmenorrhea, migraine, dental and musculoskeletal pain, and as opioid-sparing components in acute pain and perioperative care.
- Parenteral ketorolac and IV ibuprofen provide short-term management of moderate-to-severe acute pain where oral intake is limited, with strict duration limits for ketorolac due to GI and renal toxicity risks.
- Topical NSAIDs (e.g., diclofenac gel/patch) are recommended for localized soft-tissue and OA pain to reduce systemic adverse effects.
Adverse effects and toxicity
Gastrointestinal
- COX-1 inhibition reduces gastroprotective prostaglandins, increasing risk of dyspepsia, gastritis, peptic ulcer, and GI bleeding, with higher risk in older adults, prior ulcer/bleed, H. pylori infection, high doses, and concomitant anticoagulants or antiplatelets.
- COX-2 selectivity reduces endoscopic ulceration rates but does not abolish risk, and serious lower GI events still occur, particularly with concurrent aspirin.
- Misoprostol prevents NSAID-induced gastric and duodenal ulcers and reduces serious upper GI complications but is limited by dose-related diarrhea and cramping.
Renal
- NSAIDs can precipitate acute kidney injury by inhibiting prostaglandin-mediated afferent arteriolar dilation, especially in volume depletion, CKD, cirrhosis, heart failure, or with ACEI/ARB/diuretics, and can cause sodium retention, edema, hypertension, hyperkalemia, and papillary necrosis or interstitial nephritis.
- Class use is contraindicated in advanced renal failure and requires caution, dose minimization, and monitoring in renal risk states.
Cardiovascular
- Non-aspirin NSAIDs increase risk of serious cardiovascular thrombotic events, including myocardial infarction and stroke, with risk detectable within weeks of initiation and increasing with dose and duration.
- Diclofenac shows higher CV risk signals in multiple analyses, while uncertainty remains about relative safety differences across agents, emphasizing lowest effective dose for shortest duration.
- NSAIDs also roughly double heart failure hospitalizations across selective and nonselective agents, and vigilance is warranted in patients with existing CV disease.
Hepatic
- Transaminase elevations are uncommon and usually mild, but rare severe hepatotoxicity has been reported, with diclofenac carrying a higher hepatotoxicity signal among NSAIDs.
- Avoid or monitor in hepatic impairment and discontinue if jaundice or systemic hepatitis features occur.
Hematologic and hypersensitivity
- Reversible platelet inhibition by non-aspirin NSAIDs can worsen bleeding in susceptible patients or perioperatively, with additive effects alongside anticoagulants or antiplatelets.
- Hypersensitivity phenotypes include NSAID-exacerbated respiratory disease (AERD/NERD), NSAID-exacerbated cutaneous disease, and NSAID-induced urticaria/angioedema, largely driven by COX-1 inhibition shifting arachidonic acid toward leukotrienes.
- Anaphylactoid reactions can occur, and diagnosis is clinical with avoidance of cross-reactive COX-1 inhibitors and consideration of selective alternatives when necessary.
Other organ toxicity
- Mitochondrial oxidative stress and electron transport chain inhibition have been implicated in organ toxicity for some NSAIDs, with diclofenac demonstrating potent complex I inhibition in preclinical systems.
- CNS effects (headache, dizziness), photosensitivity, and aseptic meningitis (notably with ibuprofen in autoimmune disease) are recognized but less common.
Risk mitigation and gastroprotection
- Use the lowest effective dose for the shortest duration consistent with treatment goals, reassessing ongoing need regularly to minimize GI, CV, and renal risks.
- In high GI risk patients, combine a nonselective NSAID with a proton pump inhibitor or use a COX-2 selective agent with gastroprotection depending on concomitant aspirin and CV risk profile.
- Misoprostol 200 µg multiple daily dosing prevents ulcers and reduces serious upper GI complications but causes dose-limiting GI adverse effects; PPIs are effective and generally better tolerated for upper GI prevention.
Drug interactions of clinical importance
- Aspirin interaction: ibuprofen and some other NSAIDs can reduce aspirin’s irreversible platelet COX-1 binding if taken concurrently, attenuating cardioprotection; separate dosing or choose alternatives to avoid interference.
- Anticoagulants/antiplatelets/SSRIs: additive GI bleeding risk requires avoidance or protective strategies and patient counseling.
- Antihypertensives and diuretics: blunted antihypertensive response and increased risk of AKI with ACEI/ARB/diuretics necessitate monitoring and avoidance of the “triple whammy” combination when possible.
- Lithium and methotrexate: reduced renal clearance can raise concentrations and toxicity risk, calling for monitoring or alternative analgesics in high-risk regimens.
Special populations and perioperative use
- Pregnancy: contraindicated in the third trimester due to risk of premature ductus arteriosus closure and oligohydramnios, and generally avoided earlier unless benefits outweigh risks.
- Perioperative: NSAIDs provide opioid-sparing analgesia in multimodal regimens; agent, dose, and bleeding/renal risk stratification guide safe incorporation rather than blanket avoidance.
- Older adults and comorbid conditions: higher baseline GI, renal, and CV risks require conservative dosing, gastroprotection, agent selection aligned with risk, and periodic monitoring.
Agent-focused profiles (concise)
- Ibuprofen: widely used, short half-life, good analgesic/antipyretic profile, aspirin interaction consideration, GI/renal/CV class warnings apply.
- Naproxen: effective analgesic with some observational suggestions of comparatively lower CV risk, though not definitive; GI risk persists.
- Diclofenac: potent anti-inflammatory efficacy with higher CV and hepatic risk signals, requiring careful patient selection and dose minimization.
- Indomethacin: strong anti-inflammatory agent used also in specific indications (e.g., acute gout), but CNS and GI tolerability limit chronic use.
- Ketorolac: potent parenteral analgesic for short-term use only due to high GI and renal toxicity with extended durations.
- Piroxicam/oxaprozin: long half-lives permit once-daily dosing but increase cumulative GI and other risks; reserve for selected patients with risk mitigation.
- Meloxicam: preferential COX-2 at lower doses with once-daily dosing and balanced GI/CV considerations; still carries class risks.
- Celecoxib: COX-2 selective with lower upper GI risk versus nonselective agents at comparable effect, but class CV warnings apply, especially at higher doses and in high-risk patients.
- Aspirin: at analgesic doses behaves as an NSAID with GI risk, but at low doses is used primarily as an antiplatelet due to irreversible platelet COX-1 inhibition.
Practical prescribing algorithm (MBBS focus)
- For acute nociceptive pain without major comorbidity: start with ibuprofen or naproxen at the lowest effective dose for the shortest duration, adding a PPI if GI risk factors exist.
- If high GI risk but low CV risk: consider celecoxib plus a PPI, or nonselective NSAID plus PPI if coxib unsuitable, tailoring to patient risk and concomitant aspirin.
- If high CV risk or established disease: avoid or minimize NSAID use; when necessary, use the lowest dose for the shortest time with careful selection, considering naproxen in some contexts and always integrating cardioprotective strategies.
- Renal risk (CKD, ACEI/ARB/diuretic, volume depletion): avoid or limit NSAIDs, monitor renal function, and consider non-NSAID analgesics or topical NSAIDs for localized disease.
Perioperative pearls
- Incorporate NSAIDs as part of multimodal analgesia when bleeding risk, renal status, and surgical context allow, selecting agents with appropriate half-life and reversibility to balance analgesia with safety.
- Avoid NSAIDs in procedures with high bleeding risk or where renal perfusion is precarious, and coordinate dosing around neuraxial anesthesia per institutional guidance.
High-yield exam points
- NSAIDs act by COX inhibition; COX-1 supports GI cytoprotection and platelets, COX-2 mediates inflammatory prostanoids; selectivity drives GI versus CV risk trade-offs.
- Aspirin irreversibly inhibits platelet COX-1, distinguishing it from other NSAIDs and explaining its antiplatelet role in secondary prevention.
- Non-aspirin NSAIDs carry boxed warnings for increased risk of MI and stroke that can occur within weeks, and risk increases with dose and duration; use the lowest effective dose for the shortest time.
- GI risk mitigation includes PPIs or misoprostol and careful agent selection, with coxibs lowering upper GI event rates but not eliminating risk.
- Renal adverse effects are amplified in conditions dependent on prostaglandin-mediated renal perfusion, making NSAIDs hazardous in CKD, heart failure, cirrhosis, and with ACEI/ARB/diuretics.
Tables for quick reference
Table: NSAID uses and cautions
Table: Contraindications and monitoring
Suggested reading anchors (textbook alignment)
- Goodman & Gilman integrates NSAIDs within autacoids and inflammation with mechanistic and clinical pearls on COX biology and class effects.
- Katzung provides a concise, exam-oriented presentation of COX-1/COX-2 pharmacology, aspirin’s irreversible action, and class comparisons by chemistry and selectivity.
- Regulatory and practice advisories frame real-world GI/CV/renal risk management and inform dose/duration and gastroprotection decisions.
References
- Ghlichloo I, Gerriets V. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs). In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023–2025.
- Katzung BG, ed. NSAIDs, Acetaminophen, & Drugs Used in Rheumatoid Arthritis and Gout. Basic & Clinical Pharmacology. McGraw-Hill; 11th ed. online summary.
- Brunton LL, Hilal-Dandan R, Knollmann BC, eds. Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 13th ed. New York: McGraw-Hill; 2017. Section on Analgesic-Antipyretic and Anti-inflammatory Agents.
- FDA. Drug Safety Communication: FDA strengthens warning that non-aspirin NSAIDs increase chance of heart attack or stroke. 2015.
- Lanas A, et al. Adverse effects of non-steroidal anti-inflammatory drugs on the upper gastrointestinal tract: Best Pract Res Clin Gastroenterol. 2010;24(2):121–132.
- Kuźniar J, et al. Practice Advisory on the Appropriate Use of NSAIDs in Primary Care. Pain Ther. 2020;9(2):519–536.
- Raskin JB, et al. Misoprostol dosage in prevention of NSAID-induced ulcers. Arch Intern Med. 1995;155(20):2381–2387.
- Sostres C, et al. GI safety of NSAIDs and coxibs—narrative insights. Cureus Review. 2023.
- Bindu S, et al. Non-steroidal anti-inflammatory drugs and organ toxicity: a comprehensive review. Life Sci. 2020;252:117–128.
- Levy N, et al. NSAIDs in the perioperative period. BJA Educ. 2023;23(10):348–355.
- Koskela HO, et al. NSAID-exacerbated respiratory disease: population study. ERJ Open Res. 2021;7(4):00462–2021.
QUIZ: Please note that if you have any issues while attempting the quiz, either click on ‘Exit mobile version’ at the bottom of this page and redo the quiz or access it on desktops/laptops.

Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.
Community Notes
Join the Discussion
Ask follow-up questions, add clinical perspective, or share a useful clarification for the next reader.