1. Definition & Epidemiology
Ischemic heart disease (IHD)—also called coronary artery disease (CAD)—is defined by impaired blood supply (ischemia) to the myocardium, usually due to narrowing or obstruction of the coronary arteries by atherosclerotic plaque. IHD is the leading cause of morbidity and mortality worldwide, particularly affecting adults over age 40 and those with major cardiovascular risk factors.
2. Pathophysiology
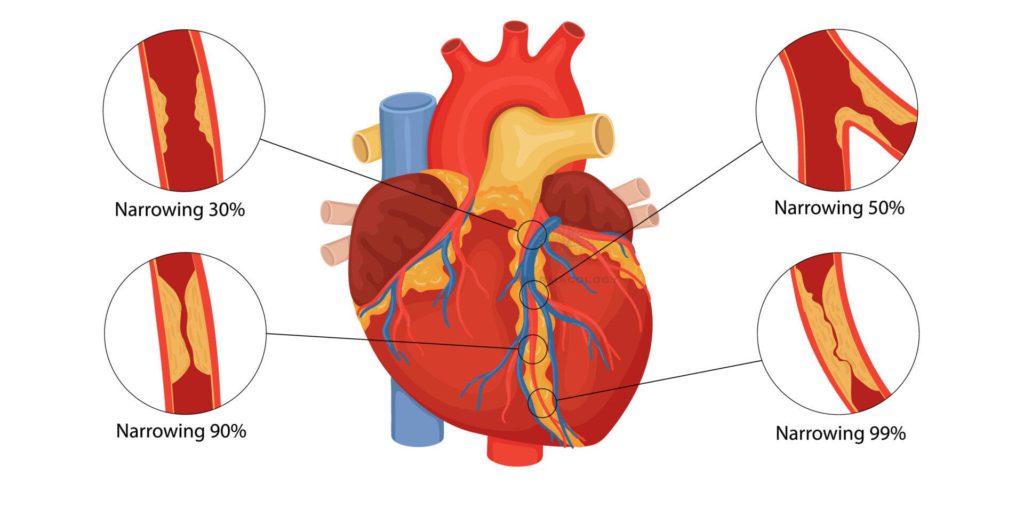
- Key Mechanism: Atherosclerosis—accumulation of cholesterol-laden plaques within coronary arteries causes luminal narrowing, reducing oxygen delivery to heart muscle.
- Acute events: Rupture of an unstable plaque with subsequent thrombus formation may cause complete occlusion, resulting in acute myocardial infarction (MI).
- Risk Factors:
- Non-modifiable: Age, male sex, family history/genetics.
- Modifiable: Hypertension, dyslipidemia, diabetes, obesity, smoking, sedentary lifestyle, stress, unhealthy diet.
3. Clinical Presentation
| Stage | Symptoms | Notes |
|---|---|---|
| Chronic stable | Exertional chest pain (angina), fatigue, shortness of breath | Symptoms relieved by rest/nitroglycerin |
| Acute coronary syndrome | Persistent chest pain, diaphoresis, nausea, palpitations | May signal MI; emergency |
| Silent ischemia | No typical angina; atypical symptoms (esp. elderly, diabetic patients) | Detected via ECG or imaging |
| Heart failure | Edema, orthopnea, dyspnea | Due to chronic ischemia |
4. Diagnostic Approach
| Test | Principle | Diagnostic Value |
|---|---|---|
| ECG | Records cardiac electrical activity | Detects ischemia, arrhythmia |
| Stress test | Monitors heart under exertion | Provokes symptoms, unmasking ischemia |
| Echocardiogram | Ultrasound imaging of heart | Assess function, motion, ejection fraction |
| Coronary angiogram | Dye and X-ray visualizes arteries | Gold standard for obstruction |
| CT/MRI coronary imaging | Noninvasive, advanced assessment | Useful for non-acute evaluation |
| Blood tests | Troponin, CK-MB, lipid/liver/kidney profiles | Confirm MI, metabolic risk |
5. Management Strategies
A. Lifestyle Modification
- Mediterranean/heart-healthy diet (limit saturated fat, cholesterol, sugar).
- Regular aerobic exercise (30–45 min most days).
- Smoking cessation.
- Weight management and stress reduction.
- Blood pressure and diabetes control.
B. Pharmacologic Therapy
| Drug Class | Examples | Purpose/Mechanism |
|---|---|---|
| Antiplatelets | Aspirin, clopidogrel | Prevent clot formation |
| Statins | Atorvastatin, rosuvastatin | Lower LDL, stabilize plaques |
| Beta-blockers | Metoprolol, atenolol | Reduce heart rate, oxygen demand |
| ACE inhibitors/ARBs | Enalapril, losartan | Lower blood pressure, prevent remodeling |
| Nitrates | Nitroglycerin | Relieve angina (vasodilation) |
| Calcium channel blockers | Diltiazem, amlodipine | Vasodilation, symptom relief |
| Newer agents | PCSK9 inhibitors, SGLT2 inhibitors (in comorbid diabetes, HF) | Reduce risk, target specific populations |
- Medication Adherence: Lifelong commitment; regular review for interactions and side effects.
C. Revascularization
| Procedure | Indication | Highlights |
|---|---|---|
| Percutaneous Coronary Intervention (PCI) | Acute MI, lifestyle-resistant angina | Balloon angioplasty ± stent placement |
| Coronary Artery Bypass Grafting (CABG) | Left main/multivessel, DM, failed PCI | Surgical rerouting using graft |
6. Follow-Up and Long-Term Care
- Regular assessment: Blood pressure, lipid profile, glycemic status, ECGs.
- Comorbidity management: Diabetes, kidney disease, arrhythmia.
- Patient education: Symptom recognition, emergency response, medication side effects.
- Cardiac rehabilitation: Supervised exercise, risk factor education, psychological support.
7. Prognosis and Prevention
- Prognosis depends on degree of vessel involvement, comorbidity control, adherence to therapy.
- Primary prevention: Risk factor control before onset.
- Secondary prevention: Aggressive intervention post-MI or diagnosis to prevent recurrence or progression.
Summary Table: Textbook Comparison of Key IHD Treatments
| Strategy | Primary Effect | Most Effective For | Key Textbook References |
|---|---|---|---|
| Lifestyle | Reduces overall CV risk | All patients, prevention | Braunwald, Harrison’s |
| Antiplatelets | Prevents acute MI | All diagnosed IHD | Katzung, G&G, NICE/ACC/AHA |
| Statins | Lower cholesterol, resolve plaques | Dyslipidemia, secondary prevention | G&G, ESC Guidelines |
| PCI | Immediate reperfusion | Acute STEMI/NSTEMI | ACC/AHA |
| CABG | Complete anatomical correction | Complex/multivessel disease | Harrison’s, ACC/AHA |
References
- Braunwald’s Heart Disease (11th Edition)
- Harrison’s Principles of Internal Medicine (21st Edition)
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics (13th Edition, Cardiac Drugs section)
- Katzung BG, Basic & Clinical Pharmacology (15th Edition)
- ACC/AHA/ESC Guidelines on management of coronary artery disease
With a patient-focused, scientifically accurate approach, this chapter brings together etiology, symptomatology, diagnostic workup, therapy, and prevention as recommended by top clinical textbooks and guidelines.
Quiz on IHD
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.
Community Notes
Join the Discussion
Ask follow-up questions, add clinical perspective, or share a useful clarification for the next reader.