Learning Objectives
By the end of this chapter, the student should be able to:
- define antiplatelet drugs
- explain the physiology of platelet activation and aggregation
- classify antiplatelet drugs
- describe the mechanism of action of major antiplatelet classes
- discuss their pharmacological actions, therapeutic uses, adverse effects, and contraindications
- distinguish antiplatelet drugs from anticoagulants
- answer common viva and university examination questions on the topic
1. Introduction
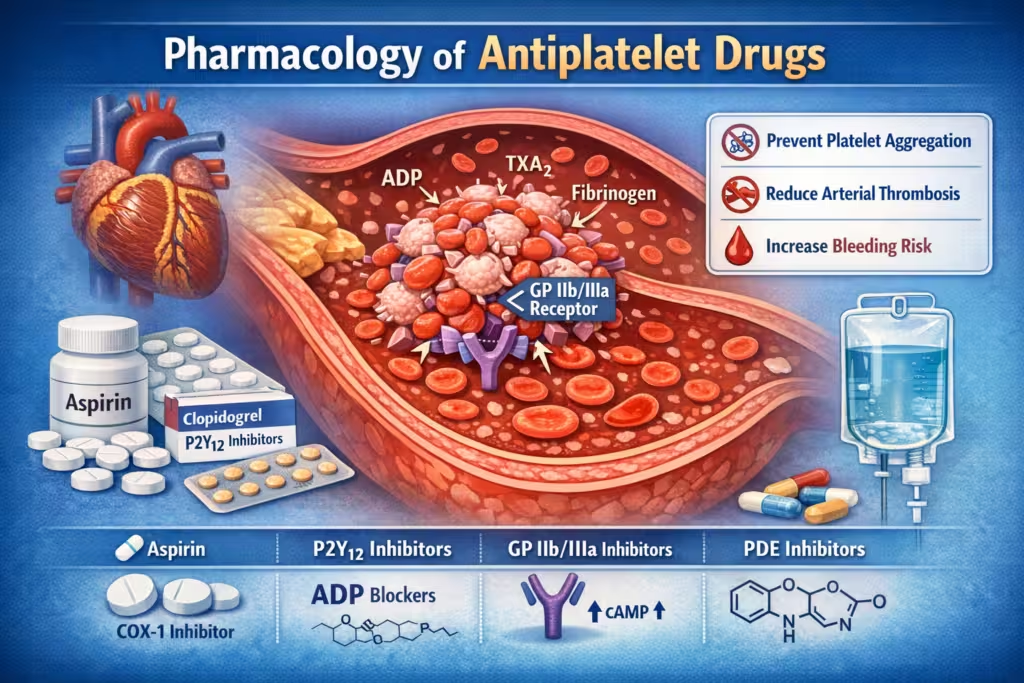
Antiplatelet drugs are agents that inhibit platelet activation, adhesion, or aggregation, thereby reducing formation of platelet-rich arterial thrombi. They are especially important in diseases such as acute coronary syndromes, myocardial infarction, ischemic stroke, transient ischemic attack, and peripheral arterial disease. Aspirin remains the classic antiplatelet drug, while P2Y12 inhibitors and GP IIb/IIIa inhibitors are central to modern therapy. (NCBI)
Antiplatelet drugs differ from anticoagulants. Antiplatelet drugs act mainly on primary hemostasis and are more useful in arterial thrombosis, whereas anticoagulants mainly inhibit the coagulation cascade and are more important in venous thrombosis and cardioembolic disease. (NCBI)
2. Physiological Basis of Platelet Aggregation
2.1 Platelet plug formation
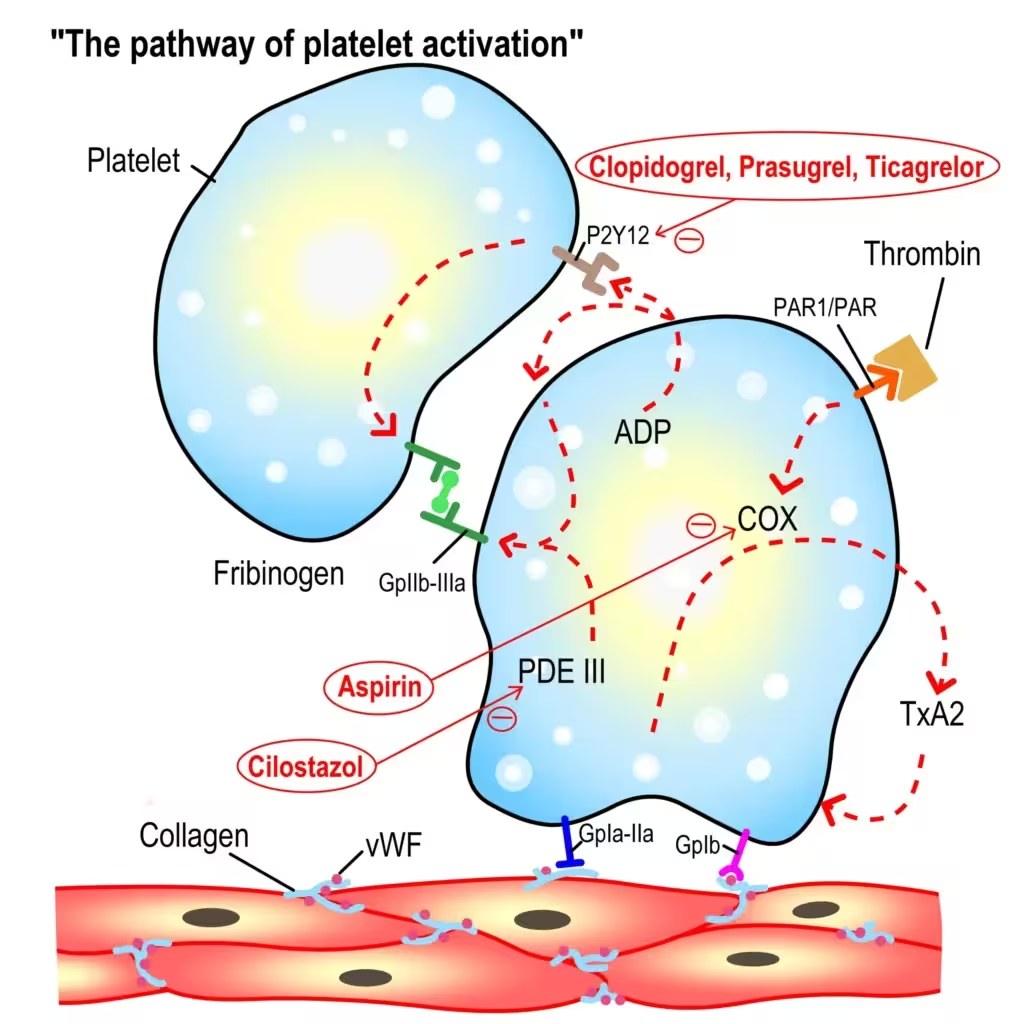
When vascular endothelium is injured, platelets first adhere to exposed subendothelial structures, then become activated, release mediators, and finally aggregate to form a platelet plug. This explains why platelet-directed drugs are so effective in preventing arterial thrombus formation. (NCBI)
2.2 Important mediators in platelet activation
Major mediators include:
- ADP
- thromboxane A₂ (TXA₂)
- thrombin
- fibrinogen bridging via GP IIb/IIIa receptors
Antiplatelet drugs work by blocking one or more of these pathways. Aspirin blocks TXA₂ formation, P2Y12 inhibitors block ADP signaling, and GP IIb/IIIa inhibitors block the final common pathway of aggregation. (NCBI)
3. Definition
Antiplatelet drugs are medications that reduce platelet function and prevent platelets from sticking together, thereby lowering the risk of arterial thrombosis. (Cleveland Clinic)
4. Classification of Antiplatelet Drugs
4.1 Cyclooxygenase inhibitor
- Aspirin
4.2 ADP (P2Y12) receptor antagonists
- Clopidogrel
- Prasugrel
- Ticagrelor
- Ticlopidine
- Cangrelor
4.3 Glycoprotein IIb/IIIa receptor antagonists
- Abciximab
- Eptifibatide
- Tirofiban
4.4 Phosphodiesterase inhibitors / adenosine-mediated drugs
- Dipyridamole
- Cilostazol
This mechanism-based grouping is standard and reflects how current antiplatelet therapy is understood clinically. (NCBI)
5. Classification Table
| Class | Drugs | Main Target |
|---|---|---|
| Cyclooxygenase inhibitor | Aspirin | COX-1 → TXA₂ synthesis |
| P2Y12 inhibitors | Clopidogrel, Prasugrel, Ticagrelor, Ticlopidine, Cangrelor | ADP receptor |
| GP IIb/IIIa inhibitors | Abciximab, Eptifibatide, Tirofiban | Final common pathway of aggregation |
| PDE / adenosine pathway drugs | Dipyridamole, Cilostazol | Increase platelet cAMP / reduce activation |
6. Aspirin
6.1 Mechanism of action
Aspirin irreversibly inhibits cyclooxygenase-1 (COX-1) in platelets, thereby reducing the formation of thromboxane A₂, which normally promotes platelet aggregation and vasoconstriction. Because platelets are anucleate, they cannot synthesize new COX, so the effect lasts for the life span of the platelet, about 7 to 10 days. (NCBI)
6.2 Pharmacological actions
- inhibits platelet aggregation
- prolongs bleeding time
- reduces arterial thrombus formation
- lowers risk of myocardial infarction and ischemic stroke
6.3 Therapeutic uses
- acute coronary syndrome
- secondary prevention after myocardial infarction
- ischemic stroke and TIA prevention
- peripheral arterial disease
- after coronary interventions in selected patients
6.4 Adverse effects
- gastric irritation
- peptic ulceration
- gastrointestinal bleeding
- hypersensitivity reactions
- bleeding tendency
6.5 Important point
Aspirin is the classical irreversible antiplatelet drug and remains a cornerstone of antiplatelet therapy. (NCBI)
7. P2Y12 Receptor Antagonists
These drugs block the P2Y12 receptor, preventing ADP-mediated platelet activation and reducing subsequent GP IIb/IIIa activation. This class is fundamental in acute coronary syndrome and dual antiplatelet therapy. (NCBI)
7.1 Clopidogrel
7.1.1 Mechanism of action
Clopidogrel is a prodrug that requires hepatic activation. Its active metabolite irreversibly blocks the P2Y12 receptor on platelets. (NCBI)
7.1.2 Uses
- acute coronary syndrome
- recent myocardial infarction
- recent ischemic stroke
- peripheral arterial disease
- post-stent therapy
7.1.3 Adverse effects
- bleeding
- rash
- diarrhea
- rare thrombotic thrombocytopenic purpura
7.2 Prasugrel
7.2.1 Mechanism of action
Prasugrel is also a prodrug and irreversibly blocks the P2Y12 receptor.
7.2.2 Key features
- faster onset than clopidogrel
- greater and more consistent platelet inhibition
- higher bleeding risk in some patients compared with clopidogrel (OUP Academic)
7.2.3 Uses
- acute coronary syndrome
- especially in PCI settings
7.3 Ticagrelor
7.3.1 Mechanism of action
Ticagrelor is a direct-acting, reversible P2Y12 inhibitor, unlike clopidogrel and prasugrel. (NCBI)
7.3.2 Adverse effects
- bleeding
- dyspnea
- bradyarrhythmia in some patients
7.4 Ticlopidine
This is an older thienopyridine now rarely used because of serious adverse effects such as:
- neutropenia
- agranulocytosis
- thrombotic thrombocytopenic purpura
7.5 Cangrelor
Cangrelor is an intravenous, reversible P2Y12 inhibitor used when rapid onset and offset are required, especially around PCI. (NCBI)
8. GP IIb/IIIa Receptor Antagonists
8.1 Mechanism of action
These drugs block the glycoprotein IIb/IIIa receptor, which is the final common pathway of platelet aggregation because fibrinogen cross-linking depends on this receptor. (StatPearls)
8.2 Drugs
- Abciximab
- Eptifibatide
- Tirofiban
8.3 Clinical uses
They are given parenterally and are mainly used in:
- acute coronary syndrome
- percutaneous coronary intervention
- selected high-risk cardiology settings (NCBI)
8.4 Adverse effects
- bleeding
- thrombocytopenia
9. Dipyridamole
9.1 Mechanism of action
Dipyridamole inhibits phosphodiesterase and interferes with adenosine uptake, increasing platelet cAMP, which reduces platelet activation.
9.2 Uses
- prevention of stroke in combination with aspirin
- selected cardiovascular uses
- pharmacologic stress testing because of vasodilator action
9.3 Adverse effects
- headache
- flushing
- dizziness
- hypotension
10. Cilostazol
10.1 Mechanism of action
Cilostazol is a phosphodiesterase III inhibitor that increases cAMP in platelets and blood vessels, causing:
- inhibition of platelet aggregation
- vasodilation
10.2 Uses
- intermittent claudication in peripheral arterial disease
10.3 Adverse effects
- headache
- palpitations
- tachycardia
- diarrhea
11. Summary Table of Major Antiplatelet Drugs
| Drug/Class | Mechanism | Reversible/Irreversible | Main Uses | Major Adverse Effect |
|---|---|---|---|---|
| Aspirin | inhibits COX-1 → ↓ TXA₂ | Irreversible | ACS, MI, stroke prevention | GI irritation, bleeding |
| Clopidogrel | blocks P2Y12 receptor | Irreversible | ACS, post-stent, stroke prevention | bleeding, rare TTP |
| Prasugrel | blocks P2Y12 receptor | Irreversible | ACS with PCI | bleeding |
| Ticagrelor | blocks P2Y12 receptor | Reversible | ACS, DAPT | bleeding, dyspnea |
| Cangrelor | blocks P2Y12 receptor | Reversible | PCI settings | bleeding |
| GP IIb/IIIa inhibitors | block final common pathway | Mostly reversible class effect, abciximab functionally prolonged | ACS, PCI | bleeding, thrombocytopenia |
| Dipyridamole | ↑ cAMP | Reversible | stroke prevention with aspirin | headache |
| Cilostazol | PDE III inhibition | Reversible | intermittent claudication | tachycardia, headache |
12. Dual Antiplatelet Therapy
12.1 Definition
Dual antiplatelet therapy means the use of:
Aspirin + a P2Y12 inhibitor
Examples include:
- aspirin + clopidogrel
- aspirin + prasugrel
- aspirin + ticagrelor
12.2 Rationale
These drugs block different platelet activation pathways, giving stronger antithrombotic protection. DAPT is a cornerstone of therapy in acute coronary syndromes and after coronary stenting. (European Society of Cardiology)
12.3 Limitation
The major problem is increased bleeding risk. (European Society of Cardiology)
13. Therapeutic Uses of Antiplatelet Drugs
13.1 Ischemic heart disease
- unstable angina
- myocardial infarction
- acute coronary syndrome
- chronic coronary artery disease
13.2 Coronary interventions
- after angioplasty
- after coronary stenting
- PCI-related antithrombotic therapy
13.3 Cerebrovascular disease
- transient ischemic attack
- secondary prevention of ischemic stroke
13.4 Peripheral arterial disease
- prevention of vascular events
- symptomatic disease management
Antiplatelet therapy is a cornerstone of pharmacologic management in coronary artery disease and other arterial thrombotic conditions. (PMC)
14. Adverse Effects of Antiplatelet Drugs
14.1 Bleeding
This is the most important adverse effect of the whole group.
It may present as:
- bruising
- gum bleeding
- epistaxis
- gastrointestinal bleeding
- intracranial hemorrhage in severe cases
14.2 Drug-specific toxicities
| Drug | Characteristic adverse effect |
|---|---|
| Aspirin | gastritis, peptic ulcer, GI bleeding |
| Clopidogrel | rare TTP |
| Prasugrel | higher major bleeding risk |
| Ticagrelor | dyspnea |
| GP IIb/IIIa inhibitors | thrombocytopenia |
| Dipyridamole | headache, flushing |
| Cilostazol | palpitations, tachycardia |
All antiplatelet classes ultimately raise bleeding risk because all reduce platelet function. (NCBI)
15. Contraindications and Precautions
Antiplatelet drugs should be used carefully or avoided in:
- active bleeding
- peptic ulcer disease
- hemorrhagic stroke
- severe thrombocytopenia
- major surgery when interruption is necessary
- severe uncontrolled hypertension in some settings
Periprocedural interruption requires balancing bleeding risk against thrombotic risk, especially in patients with recent coronary stents. (PMC)
16. Antiplatelet Drugs versus Anticoagulants
| Feature | Antiplatelet Drugs | Anticoagulants |
|---|---|---|
| Main target | platelets | coagulation factors |
| Best for | arterial thrombosis | venous thrombosis, cardioembolism |
| Thrombus type | platelet-rich | fibrin-rich |
| Examples | aspirin, clopidogrel | heparin, warfarin, DOACs |
16.1 Key concept
Arterial thrombi are mainly platelet-rich, so antiplatelet drugs are especially useful there. (NCBI)
17. Mnemonics
17.1 Aspirin
“Aspirin Abolishes A₂”
Aspirin abolishes thromboxane A₂.
17.2 Clopidogrel
“CLOP closes the P2Y12 door.”
17.3 Ticagrelor
“Tica is quick and reversible.”
17.4 GP IIb/IIIa blockers
“ATE the fibrin bridge”
- Abciximab
- Tirofiban
- Eptifibatide
17.5 DAPT
“A + P = Powerful Platelet Prevention”
Aspirin + P2Y12 inhibitor
18. High-Yield Exam Points
- Aspirin irreversibly inhibits platelet COX-1 and reduces TXA₂. (NCBI)
- Clopidogrel and prasugrel are irreversible P2Y12 inhibitors; ticagrelor is reversible. (NCBI)
- GP IIb/IIIa inhibitors block the final common pathway of platelet aggregation. (StatPearls)
- Main adverse effect of all antiplatelet drugs is bleeding. (NCBI)
- Antiplatelet drugs are mainly used in arterial thrombosis. (Cleveland Clinic)
- Cilostazol is used in intermittent claudication.
- DAPT is standard in ACS and after coronary stenting. (European Society of Cardiology)
19. Viva Questions and Answers
19.1 Short viva questions
1. What are antiplatelet drugs?
They are drugs that inhibit platelet activation or aggregation and prevent arterial thrombus formation.
2. Which is the most common antiplatelet drug?
Aspirin.
3. How does aspirin act as an antiplatelet drug?
It irreversibly inhibits COX-1 and decreases TXA₂ synthesis.
4. Which receptor is blocked by clopidogrel?
P2Y12 receptor.
5. Is clopidogrel a prodrug?
Yes.
6. Which P2Y12 inhibitor is reversible?
Ticagrelor.
7. Which antiplatelet drugs block the final common pathway?
GP IIb/IIIa inhibitors.
8. Name an intravenous P2Y12 inhibitor.
Cangrelor.
9. Which drug is used for intermittent claudication?
Cilostazol.
10. What is the major adverse effect of antiplatelet drugs?
Bleeding.
19.2 Long viva questions
1. Classify antiplatelet drugs and explain the mechanism of action of each class.
2. Write a detailed note on aspirin as an antiplatelet drug.
3. Compare clopidogrel, prasugrel, and ticagrelor.
4. What are GP IIb/IIIa inhibitors? Discuss their uses and adverse effects.
5. Differentiate antiplatelet drugs from anticoagulants.
20. Short Notes for University Examinations
20.1 Short note: Aspirin as an antiplatelet drug
Aspirin irreversibly inhibits platelet COX-1 and suppresses thromboxane A₂ formation. It inhibits platelet aggregation for the life span of the platelet. It is used in ACS, MI, stroke prevention, and post-stent states. Major adverse effects are gastritis, peptic ulceration, and bleeding. (NCBI)
20.2 Short note: Clopidogrel
Clopidogrel is a prodrug that irreversibly blocks the platelet P2Y12 receptor after hepatic activation. It is used in ACS, stroke prevention, peripheral arterial disease, and after coronary stenting. Major adverse effect is bleeding; rare TTP may occur. (NCBI)
20.3 Short note: GP IIb/IIIa inhibitors
These drugs block the final common pathway of platelet aggregation by inhibiting fibrinogen binding to the GP IIb/IIIa receptor. They are used intravenously in ACS and PCI. Major adverse effects are bleeding and thrombocytopenia. (StatPearls)
21. One-Page Revision Table
| Topic | Key Point |
|---|---|
| Best for | arterial thrombosis |
| Classical drug | aspirin |
| Aspirin action | irreversible COX-1 inhibition |
| Clopidogrel | irreversible P2Y12 blocker, prodrug |
| Ticagrelor | reversible P2Y12 blocker |
| Final common pathway blockers | GP IIb/IIIa inhibitors |
| Drug for intermittent claudication | cilostazol |
| Main toxicity | bleeding |
| DAPT | aspirin + P2Y12 inhibitor |
22. Conclusion
Antiplatelet drugs are central to the prevention and treatment of atherothrombotic cardiovascular and cerebrovascular disease. Their pharmacology revolves around blocking key platelet pathways, especially TXA₂ synthesis, ADP signaling, and GP IIb/IIIa-mediated aggregation. A solid understanding of their classification, mechanism, clinical uses, and adverse effects is essential for MBBS students because these are among the most important drugs in modern medicine. (NCBI)
23. Rapid Recall Box
- Aspirin → irreversible COX-1 inhibitor
- Clopidogrel / Prasugrel → irreversible P2Y12 blockers
- Ticagrelor → reversible P2Y12 blocker
- Cangrelor → IV reversible P2Y12 blocker
- Abciximab / Eptifibatide / Tirofiban → GP IIb/IIIa blockers
- Dipyridamole / Cilostazol → increase cAMP, reduce platelet activation
- Main adverse effect → bleeding
- Main use → arterial thrombosis
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.
Community Notes
Join the Discussion
Ask follow-up questions, add clinical perspective, or share a useful clarification for the next reader.