Introduction
Epilepsy is a chronic neurological disorder defined by recurrent, unprovoked seizures resulting from abnormal excessive or synchronous neuronal activity in the brain. Antiepileptic drugs (AEDs), now more accurately known as anti-seizure medications (ASMs), are used both for symptomatic seizure control and, in some cases, for prevention of epileptogenesis following brain injury. Since the discovery of phenobarbital and phenytoin, AED development has led to over 30 agents, each with unique mechanisms, clinical application profiles, and adverse effects.
Classification and Mechanisms of Action
AEDs are classified by chemical structure, mechanism, or generation (older vs. newer), but mechanistic grouping aids understanding of therapeutic strategy, polytherapy, and cross-toxicity.
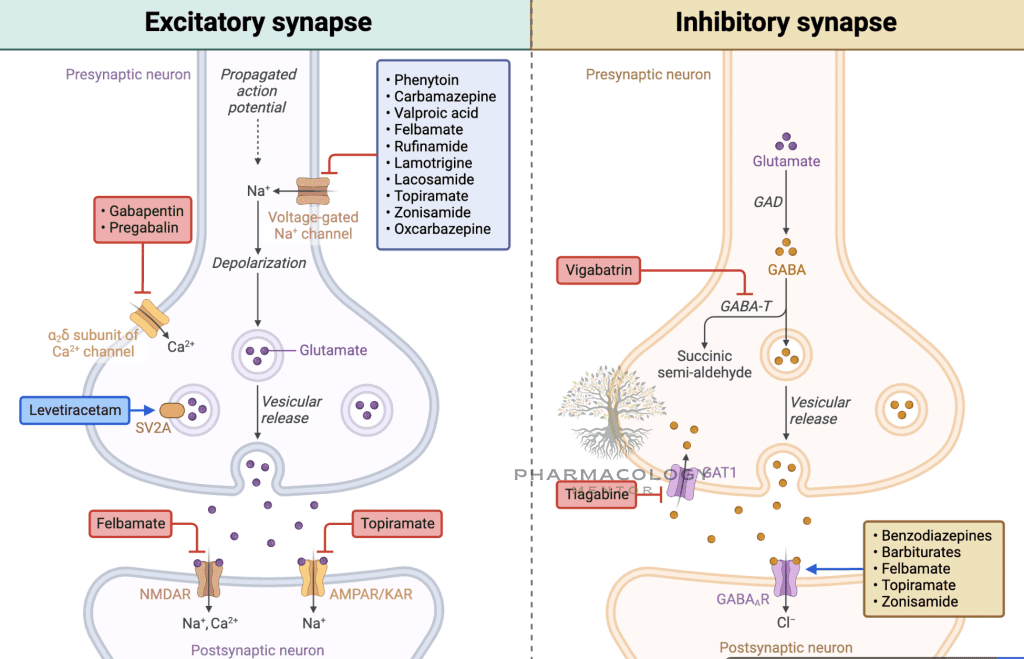
1. Modulators of Voltage-Gated Sodium Channels
Mechanism:
Block state-dependent (usually open or inactivated) voltage-gated sodium channels, inhibiting sustained high-frequency neuronal firing. They stabilize inactive states, limit seizure propagation.
Drugs and Major Uses:
- Phenytoin: Focal, generalized tonic-clonic (GTC), status epilepticus.
- Carbamazepine: Focal, GTC, trigeminal neuralgia, bipolar disorder.
- Oxcarbazepine, Eslicarbazepine: Focal.
- Lamotrigine: Focal, GTC, absence, bipolar disorder.
- Lacosamide, Rufinamide, Zonisamide: Focal (lac); LGS for ruf, generalized and focal for zon.
Adverse Effects:
Diplopia, ataxia, nystagmus, sedation (less with lamotrigine/lacosamide); hyponatremia (CBZ/OXC/ESC); rash (lamotrigine); gingival hyperplasia, hirsutism (phenytoin); hepatotoxicity (rare).
2. Drugs Enhancing GABAergic Neurotransmission
Mechanisms:
- Increase GABA synthesis/release: Valproic acid.
- Inhibit GABA degradation: Vigabatrin (irreversible GABA-transaminase inhibitor), tiagabine (blocks GABA reuptake).
- Direct GABA-A receptor agonism: Phenobarbital, benzodiazepines (BDZ; diazepam, lorazepam, clonazepam, clobazam).
Drugs/Uses:
- Valproate: GTC, absence, myoclonic, migraine, bipolar—broadest spectrum.
- BDZs: Status epilepticus (acute IV therapy), myoclonic and absence seizures.
- Barbiturates: Phenobarbital (third-line, especially in young children, status).
- Others: Tiagabine (adjunct), vigabatrin (infantile spasms, refr. focal).
Adverse Effects:
Sedation (BDZ, PHB), dependence, paradoxical excitation (children), hepatotoxicity (VPA), visual field defects (VGB—must monitor vision).
3. Calcium Channel Modulators
Mechanisms:
- T-Type Ca2+ channel inhibition: Ethosuximide (selective for thalamic oscillations in absence seizures).
- High-voltage activated Ca2+ channels: Gabapentin, pregabalin (both also treat neuropathic pain).
Drugs/Uses:
- Ethosuximide: Absence seizures (drug of choice).
- Gabapentin/Pregabalin: Adjunctive in focal, neuropathic pain, anxiety (pregabalin in GAD).
Adverse Effects:
Ethosuximide (GI upset, fatigue), rarely blood dyscrasia/SJS; GBP/PGB (somnolence, dizziness, weight gain, edema).
4. Glutamate Receptor Antagonists and Other Mechanisms
Topiramate, Felbamate, Perampanel inhibit AMPA/kainate; felbamate also antagonizes NMDA and potentiates GABA.
Levetiracetam, Brivaracetam: SV2A protein binders—unique mechanism, broad efficacy, few interactions.
Perampanel: Noncompetitive AMPA antagonist, adjunct for focal, GTC, myoclonic seizures.
Adverse Effects:
Topiramate (word-finding difficulty, weight loss, kidney stones, paresthesia); felbamate (aplastic anemia, liver failure—reserved for refractory).
5. Mixed or Multifactorial Mechanisms
Valproate: Multiple actions—blocks Na channels, increases GABA, inhibits T-type Ca2+.
Zonisamide: Blocks Na and T-type Ca2+ channels; carbonic anhydrase inhibitor.
Spectrum of Activity—Partial, Generalized, and Special Syndromes
Focal (Partial) Seizures (with or without secondary generalization)
- First generation: Carbamazepine, phenytoin, phenobarbital, primidone
- Newer: Lamotrigine, levetiracetam, oxcarbazepine, lacosamide, gabapentin, topiramate, zonisamide, pregabalin, brivaracetam
Generalized Tonic-Clonic Seizures
- Drugs: Valproic acid, lamotrigine, topiramate, levetiracetam, phenobarbital
Absence Seizures
- Drugs: Ethosuximide (first-line), valproate, lamotrigine
Myoclonic Seizures
- Drugs: Valproic acid, levetiracetam, clonazepam, topiramate
Lennox-Gastaut Syndrome (LGS)
- Drugs: Lamotrigine, topiramate, rufinamide, clobazam, felbamate, valproate, cannabidiol
Status Epilepticus
- Acute: BDZs (IV lorazepam, diazepam, midazolam, clonazepam), phenytoin/fosphenytoin, valproate, phenobarbital, levetiracetam.
Pharmacokinetics
- Absorption: Most AEDs orally well absorbed; some require slow titration (lamotrigine, topiramate) due to risk of rash/CNS effects.
- Distribution: Highly protein-bound (phenytoin, valproate, carbamazepine).
- Metabolism: Hepatic CYP-mediated (most older AEDs); newer AEDs (levetiracetam, gabapentin, pregabalin) are renally excreted and less interactive.
- Autoinduction: Carbamazepine induces its own metabolism.
Therapeutic Drug Monitoring (TDM):
Required for phenytoin, carbamazepine, phenobarbital, valproate, ethosuximide (narrow therapeutic windows; non-linear kinetics for phenytoin).
Adverse Effects of Antiepileptic Drugs
CNS Effects
- Sedation, dizziness, ataxia, diplopia, nystagmus, cognitive slowing (most AEDs).
- Idiosyncratic psychiatric/behavioral (levetiracetam: irritability, aggression).
Systemic Effects
- Rash, SJS/TEN: Lamotrigine, carbamazepine, phenytoin (Black box warning for Asian HLA-B*1502 gene).
- Blood dyscrasias: CBZ, OXC, phenytoin, ethosuximide.
- Hepatotoxicity: VPA (especially in children), felbamate, carbamazepine.
- Weight: Gain (VPA, pregabalin, gabapentin); loss (topiramate, zonisamide, felbamate).
- Renal stones, metabolic acidosis: Topiramate, zonisamide.
- Visual field defects: Vigabatrin (permanent, must monitor).
Teratogenicity
- Valproate (highest risk): Neural tube defects (spina bifida), cognitive impairment, facial dysmorphism.
- Phenytoin: Fetal hydantoin syndrome.
- Carbamazepine: NTDs, minor defects.
- Lamotrigine, levetiracetam, oxcarbazepine: Lower risk but not zero.
Best practice: Monotherapy at the lowest effective dose, high-dose folic acid supplementation for women of childbearing age.
Pharmacological Interactions
- Enzyme Inducers: Phenytoin, phenobarbital, carbamazepine, primidone—accelerate metabolism of AEDs, OCPs, warfarin, steroids, other drugs.
- Enzyme Inhibitors: Valproate; increases lamotrigine, carbamazepine epoxide, phenobarbital, ethosuximide.
- Newer AEDs: Most (e.g., levetiracetam, brivaracetam, gabapentin, pregabalin) have negligible hepatic interactions.
Always check interaction potential before adding AEDs, especially in polytherapy or patients on OCPs/anticoagulants.
Special Clinical Considerations
Drug Selection Principles
- Seizure type/syndrome
- Age, comorbidities, reproductive potential
- Adverse effect profile
- Drug interactions
- Patient preferences/adherence potential
Discontinuation
- Slow (months); abrupt withdrawal can precipitate withdrawal seizures, status epilepticus.
Non-Epilepsy Indications for AEDs
- Mood stabilization: Valproate, carbamazepine, lamotrigine in bipolar disorder.
- Neuropathic pain/fibromyalgia: Gabapentin, pregabalin, carbamazepine (trigeminal neuralgia).
- Migraine prophylaxis: Topiramate, valproate.
- Anxiety, movement disorders: Clonazepam, pregabalin, levetiracetam.
Drugs in Focus: Pearls for Leading AEDs
Phenytoin
- Non-linear kinetics; uses: seizure, status, arrhythmias.
- Toxicity: gum hypertrophy, hirsutism, neuropathy, SJS.
Carbamazepine
- Drug of choice for trigeminal neuralgia; prone to SIADH, SJS (Asians—HLA-B*1502).
Valproic Acid
- Broadest efficacy, rapid titration; avoid in pregnancy, <2 yrs, hepatic disease.
Lamotrigine
- Useful for bipolar depression, slow titration crucial; SJS risk.
Levetiracetam
- Rapid onset, renally cleared; behavioral side effects (rare serious).
Topiramate
- Broad spectrum, used in migraine; can cause weight loss, cognitive effects, kidney stones.
Future Directions and Personalized Therapy
- Precision medicine: Pharmacogenomics (HLA genotyping, CYP polymorphisms).
- Novel agents: Cannabidiol (LGS, Dravet), fenfluramine, new SV2A ligands.
- Device therapy: Vagal nerve stimulation, deep brain stimulation, responsive neurostimulation in refractory epilepsy.
Guideline Recommendations (NICE/ILAE/NeuroSocieties)
- Newly diagnosed focal epilepsy: Lamotrigine, levetiracetam, carbamazepine, or oxcarbazepine as first-line.
- Generalized seizures: Valproate (avoid in women of childbearing potential), lamotrigine, levetiracetam, topiramate.
- Absence: Ethosuximide or valproate.
- Status epilepticus: IV benzodiazepines (lorazepam) first, then phenytoin/fosphenytoin, valproate, phenobarbital, or levetiracetam.
Conclusion
Effective epilepsy management relies on tailored AED selection, vigilant safety/interaction monitoring, patient-centric care, and ongoing therapeutic adjustment. New drugs and alternative therapies continue to improve patient outcomes, but detailed knowledge of AED pharmacodynamics, kinetics, and clinical application remains the cornerstone of high-quality epilepsy care.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Ed.
- Katzung BG, Basic & Clinical Pharmacology, 15th Ed.
- Rang HP, Dale MM, Ritter JM. Rang & Dale’s Pharmacology, 9th Ed.
- Trevor AJ, Katzung BG. Review of Medical Pharmacology, 14th Ed.
- NICE Epilepsy Guidelines (NG217, 2022).
- ILAE 2018 Practical Clinical Definition/ Classification of Seizures/Epilepsies.
- Epilepsy Foundation Clinical Protocols.
- Harrison’s Principles of Internal Medicine, 21st Ed.
- Relevant FDA drug labeling and pharmacovigilance bulletins.
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.
Community Notes
Join the Discussion
Ask follow-up questions, add clinical perspective, or share a useful clarification for the next reader.