Essential medicines are drugs selected to meet the priority health care needs of a population, chosen on the basis of public‑health relevance, comparative efficacy and safety, cost‑effectiveness, and assured quality, forming the backbone of rational therapeutics, teaching, and formulary systems. Standard pharmacology textbooks present essential medicines as a framework that links evidence‑based drug selection with standard treatment guidelines, generic prescribing, bioequivalence, and reliable supply to maximize equitable access and clinical value.
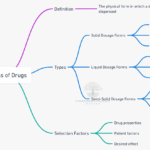
Definition and scope
Essential medicines are a curated subset of drugs intended to be available at all times in adequate amounts, appropriate dosage forms, assured quality, and at prices individuals and health systems can afford, with selection driven by disease burden and high‑quality evidence on benefit–risk and value. In teaching texts, the essential‑medicines approach underpins rational prescribing, emphasizes generic (INN) names, and aligns with formularies and standard treatment guidelines for common conditions across levels of care.
Core principles
- Public health relevance: drugs address prevalent, serious, or preventable conditions in the specific health system context, prioritizing broad clinical impact over marginal gains.
- Evidence of efficacy and safety: comparative clinical data and long experience are preferred, with clear therapeutic roles and predictable adverse‑effect profiles.
- Cost‑effectiveness and feasibility: total system costs (procurement, monitoring, delivery) and logistic feasibility (storage, stability, training needs) inform final selection.
- Assured quality and interchangeability: quality standards, generic naming, and bioequivalence underpin safe substitution and reliable therapeutic performance.
Why essential medicines matter
- Clinical outcomes: standardization around well‑studied medicines improves guideline adherence, dosing accuracy, and pharmacovigilance, reducing preventable harm from irrational polypharmacy.
- Access and equity: concentrated procurement and generic use lower prices and stabilize supply, improving availability in primary care and public facilities.
- Education and stewardship: focusing curricula on essential drugs deepens mastery of “P‑drugs” (personal drugs) and critical appraisal skills that translate into safer prescribing.
Selection criteria (textbook perspective)
- Disease burden and therapeutic priority (e.g., anti‑infectives for common community and hospital pathogens, cardiovascular risk reduction, maternal‑child health).
- Comparative effectiveness within a class (choosing a representative that covers the widest indications with favorable safety and interaction profile).
- Safety in special populations (pregnancy, pediatrics, geriatrics, renal/hepatic impairment) and need for monitoring or laboratory support.
- Cost and availability of quality‑assured generics, with bioequivalence as the operational guarantor of interchangeability.
Implementation pillars
- National essential medicines lists (NEMLs): country‑adapted lists that reflect local epidemiology, resources, and health‑system capacity, updated periodically as evidence and needs evolve.
- Standard treatment guidelines (STGs): condition‑specific protocols that operationalize essential‑medicine choices for first‑ and second‑line therapy, dose, duration, and monitoring.
- Formularies and INN prescribing: institutional formularies derived from the NEML favor INN names, therapeutic interchange, and class‑based restrictions to reduce duplication and confusion.
- Procurement and supply: centralized, quality‑assured purchasing and inventory control to ensure continuous availability and reduce stock‑outs.
- Quality, bioequivalence, and pharmacovigilance: testing, bioequivalence standards, and adverse‑event reporting sustain confidence and enable safe generic substitution.
Essential medicines across systems (illustrative classes)
- Analgesics and anti‑inflammatories: paracetamol and selected NSAIDs for nociceptive pain and fever with gastroprotection strategies where indicated.
- Anti‑infectives: representative beta‑lactams, macrolides, antituberculars, antimalarials, and antifungals selected for local susceptibility patterns and stewardship.
- Cardiovascular: diuretics, ACE inhibitors/ARBs, beta‑blockers, CCBs, statins, and antiplatelets for hypertension, ischemic disease, and heart failure.
- Endocrine and metabolic: human insulins, metformin, sulfonylureas, levothyroxine, and corticosteroids with dosing and monitoring frameworks.
- Respiratory: bronchodilators and inhaled corticosteroids for asthma/COPD with device‑based instruction integrated into STGs.
- Gastrointestinal: proton‑pump inhibitors, H2‑antagonists, antiemetics, oral rehydration salts, and laxatives with clear indications and durations.
- Hematology: oral iron, folate, vitamin B12, and anticoagulants for defined indications with lab monitoring guidance as needed.
Table: Essential medicines selection—textbook criteria and rationale
Generic names, bioequivalence, and interchangeability
Textbooks stress prescribing by INN to avoid brand confusion, encourage competition, and facilitate stewardship, while recognizing that pharmaceutical equivalents must demonstrate bioequivalence to be substitutable without compromising efficacy or safety. Clinicians should anticipate formulation‑related differences in absorption rate and tolerability and respond to patient feedback during therapeutic interchange within the same INN.
Rational use and the “P‑drug” concept
Rational use integrates problem definition, therapeutic objectives, selection of a P‑drug (the prescriber’s personal first‑choice essential medicine for a condition), verification of suitability for the individual, clear instructions, and monitoring for effect and harm. Embedding P‑drug reasoning in curricula aligns daily prescribing with essential‑medicine lists and standard treatment guidelines, improving safety and adherence.
Advantages and limitations
- Advantages: improved access, affordability, standardization, and teaching focus with reduced duplication and irrational combinations.
- Limitations: requires continuous evidence review, resistance to change from brand marketing, and adaptation to local resistance patterns and comorbidities.
Roles for education and practice
- Education: core drug lists structure MBBS teaching around mechanisms, indications, dosing, and monitoring of high‑value agents across specialties.
- Practice: formularies and STGs derived from essential‑medicine principles reduce variation, support audit and feedback, and guide procurement and pharmacovigilance.
Table: From essential medicines to bedside—linking list, guideline, and prescription
Governance, access, and quality
Sustainable essential‑medicine programs require transparent selection processes, periodic review, quality assurance of generics, supply‑chain reliability, and active pharmacovigilance to maintain public and clinician trust. Textbooks emphasize that generics are acceptable substitutes when bioequivalence is shown, anchoring formulary policies that balance cost savings with clinical performance.
High‑yield MBBS takeaways
- Essential medicines are selected for priority conditions using evidence of efficacy, safety, value, and quality; they anchor formularies, guidelines, and teaching.
- Prescribe by INN and apply bioequivalence principles to support safe generic substitution and stewardship.
- Use P‑drug reasoning and standard treatment guidelines to link essential‑medicine selection with individualized, monitored care.
References
- Tripathi KD. Essentials of Medical Pharmacology. 6th ed. New Delhi: Jaypee Brothers Medical Publishers; 2008. Rational use and essential medicines.
- Katzung BG, Masters SB, Trevor AJ. Basic & Clinical Pharmacology. Section I: Basic Principles; Rational prescribing and drug selection. New York: McGraw‑Hill; various eds.
- Ritter JM, Flower R, Henderson G, Loke YK, MacEwan D, Robinson E, Fullerton J. Rang & Dale’s Pharmacology. 9th–10th eds. London: Elsevier; General principles and rational therapeutics.
- Brunton LL, Parker KL, Blumenthal DK, Buxton ILO. Goodman & Gilman’s Manual of Pharmacology and Therapeutics. Section I: General Principles; bioavailability, bioequivalence, and formularies. New York: McGraw‑Hill; 2008.
📚 AI Pharma Quiz Generator
🎉 Quiz Results
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.