
Introduction
Erectile dysfunction (ED), defined as the consistent or recurrent inability to attain or maintain an erection sufficient for satisfactory sexual performance, affects millions of men worldwide. Though once considered an inevitable part of aging, ED is now regarded as a potentially reversible condition with multiple underlying causes, including vascular, neurogenic, hormonal, and psychogenic factors. Advances in pharmacotherapy have dramatically improved outcomes for men with ED, with novel agents and combination approaches continually expanding the therapeutic landscape.
This comprehensive review explores the pharmacotherapy of erectile dysfunction, integrating principles from Goodman & Gilman’s The Pharmacological Basis of Therapeutics, Katzung’s Basic & Clinical Pharmacology, and Rang & Dale’s Pharmacology. Topics include an overview of the physiology of penile erection, the role of phosphodiesterase type 5 (PDE5) inhibitors, alternative or adjunct treatments (e.g., prostaglandins, hormonal therapy, injectables), potential drug interactions, contraindications, and emerging therapies.
Physiology of Penile Erection
Vascular and Neurological Components
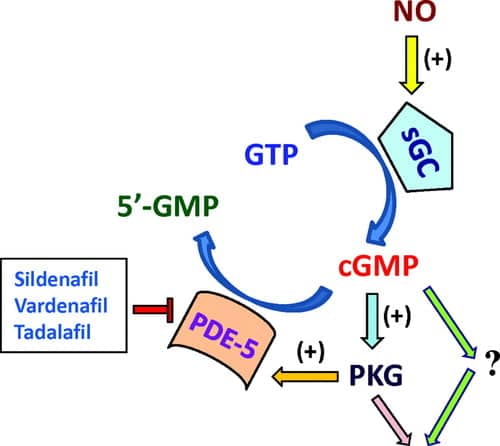
Penile erection depends on an orchestrated interplay of neural, vascular, and smooth muscle events. Sexual stimulation (central or peripheral) triggers parasympathetic outflow from the sacral spinal cord (S2-S4), resulting in the release of nitric oxide (NO) from nonadrenergic-noncholinergic (NANC) nerve terminals. NO, in turn, stimulates the production of cyclic guanosine monophosphate (cGMP) in vascular smooth muscle cells, leading to smooth muscle relaxation, arterial dilatation, and engorgement of erectile tissues (corpora cavernosa).
Role of cGMP and PDE5
Within the corpus cavernosum, cGMP signals a cascade reducing intracellular calcium concentrations and prompting vasorelaxation. However, phosphodiesterase type 5 (PDE5) breaks down cGMP into GMP, thus attenuating the erection process. Pharmacologically inhibiting PDE5 preserves cGMP levels, prolonging vasodilation and facilitating erection.
Endothelial and Hormonal Influences
Healthy endothelial function is a major predictor of erectile health, as atherosclerosis or endothelial damage impairs NO-mediated vasodilation. Similarly, testosterone plays a modulatory role in sexual desire and erectile function, with hypogonadism contributing to ED. These elements underscore why ED is sometimes an early marker of systemic vascular disease or endocrine dysfunction.
Etiologies and Evaluation
Common Causes of ED
- Vascular Conditions: Atherosclerosis, hypertension, coronary artery disease.
- Neurological Disorders: Spinal cord injuries, neuropathies (e.g., diabetic neuropathy).
- Endocrine/Hormonal: Hypogonadism (low testosterone), hyperprolactinemia.
- Psychological Factors: Performance anxiety, depression, relationship problems.
- Medications: Certain antihypertensives (especially older beta-blockers, diuretics), antidepressants, antipsychotics.
Diagnostic Approaches
A thorough history, physical examination, and appropriate laboratory tests (fasting glucose, lipid profile, serum testosterone) help identify reversible risk factors. Questionnaires (e.g., International Index of Erectile Function) quantify severity and treatment response. Penile Doppler ultrasonography or nocturnal penile tumescence testing may be considered if needed.
Phosphodiesterase Type 5 (PDE5) Inhibitors
Mechanism of Action
PDE5 inhibitors block the PDE type 5 enzyme predominantly found in the corpus cavernosum, preventing the breakdown of cGMP. By preserving cGMP levels, these agents potentiate the endogenous NO/cGMP pathway triggered by sexual stimulation, thus enhancing and prolonging penile erection. They require intact sexual stimulation to be effective—no libido or direct pro-erectile effect occurs without arousal.
Agents
Sildenafil (Viagra)
- Onset/Duration: Effective within 30–60 minutes; lasts about 4–5 hours. Absorption may be delayed by high-fat meals.
- Dosing: Typically 50 mg initially, range 25–100 mg PRN.
- Metabolism: Hepatic (CYP3A4, CYP2C9).
- Adverse Effects: Headache, flushing, dyspepsia, nasal congestion. Visual disturbances (blue-tinged vision) due to PDE6 inhibition in retina (Goodman & Gilman’s).
Tadalafil (Cialis)
- Profile: Longer half-life (~17.5 hours), enabling up to 36-hour window of efficacy.
- Dosing: 10–20 mg PRN or 2.5–5 mg daily for men desiring spontaneity.
- Uncommon side effect: Myalgia or back pain due to PDE11 inhibition.
- Food effect: Minimal impairment by meals.
Vardenafil (Levitra)
- Similar onset and duration to sildenafil (~4–5 hours).
- Dosing: 10 mg as initial dose, adjustable (5–20 mg).
- Distinct considerations: ODT (orally disintegrating tablet) formulation for convenience.
- Possible QT prolongation risk, caution with Class IA/III antiarrhythmics.
Avanafil (Stendra)
- Newer PDE5 inhibitor, rapid onset (~15–30 minutes).
- Duration: ~6 hours.
- Dosing: 50–200 mg ~15 minutes before intercourse.
- Tolerability: Similar to other PDE5 inhibitors, with headache, flushing, nasal congestion.
Contraindications and Interactions
- Nitrate Therapy: Co-administration with nitrates (e.g., nitroglycerin, isosorbide) can cause severe hypotension. Must avoid PDE5 inhibitors in patients who regularly take nitrates.
- Alpha-blockers: Risk of orthostatic hypotension if combined. Separate dosing or use selective alpha-1A blockers can mitigate risk.
- CYP3A4 Inhibitors: Ritonavir, ketoconazole, etc., increase PDE5 inhibitor plasma levels, necessitating dose adjustment to avoid toxicity.
- Adverse Effects: Headaches, flushing, lightheadedness, rarely priapism (seek medical attention for erections >4 hours).
Patient Satisfaction and Efficacy
PDE5 inhibitors generally demonstrate high success rates (70–80% improvement in mild-to-moderate ED). Patients with more complex etiologies (e.g., diabetes, post-prostatectomy) may see reduced efficacy. Regular follow-up and dose titration optimize outcomes.
Second-Line Therapies
Alprostadil (Prostaglandin E1)
Alprostadil acts via increased intracellular cAMP, relaxing smooth muscle in corpora cavernosa. Administration routes include:
- Intracavernosal Injection (Caverject): Dose range 2.5–20 µg. Erection occurs in 5–15 minutes.
- Intraurethral Suppository (MUSE): Less invasive, but reduced efficacy vs. injection.
Adverse effects: Penile pain, priapism, local fibrosis. Alprostadil often used if PDE5 inhibitors fail or are contraindicated.
Vacuum Erection Devices (VEDs)
While not pharmacological per se, VEDs create negative pressure around the penis, drawing blood into corpora cavernosa. A constriction ring maintains the erection. Can be combined with PDE5 inhibitors or intracavernosal injections. Side effects include bruising, discomfort, and potential dissatisfaction for both partners.
Androgen Replacement Therapy (ART)
Testosterone therapy is primarily indicated in ED patients with documented hypogonadism (low serum testosterone + clinical symptoms). Restoring physiologic testosterone levels may improve libido and facilitate PDE5 inhibitor response. Delivery forms: transdermal gels/patches, intramuscular injections (e.g., testosterone enanthate), subcutaneous implants. Monitor hematocrit, PSA, and lipid changes.
Papaverine and Phentolamine Injections
- Papaverine: A nonselective PDE inhibitor, relaxing smooth muscle.
- Phentolamine: An alpha-adrenergic antagonist.
Combination intracavernosal injections were used historically but overshadowed by PDE5 inhibitors and alprostadil monotherapy. Risk includes priapism, corporal fibrosis.
Future and Adjunctive Approaches
Melanocortin Receptor Agonists (e.g., Bremelanotide)
Modulating the central melanocortin pathways can influence sexual arousal. Bremelanotide, a melanocortin receptor agonist, has garnered interest for female sexual dysfunction but also has potential benefits in ED. Administered subcutaneously on-demand, though data remain limited.
Low-Intensity Shockwave Therapy (Li-ESWT)
Non-pharmacological approach: shockwaves stimulate neovascularization of penile tissue, theoretically enhancing blood flow and endothelial function. Studies show promise in mild-to-moderate ED, especially in PDE5 nonresponders. Not yet standard of care globally.
Gene Therapy and Growth Factors
Experimental strategies target nitric oxide synthase gene delivery or using gene vectors to promote tissue regeneration in corpora cavernosa. Though promising in animal models, these remain investigational in humans.
Apomorphine (Dopamine Receptor Agonist)
Previously considered for ED, apomorphine (a D1/D2 dopamine agonist) can stimulate erection via central mechanisms. Sublingual formulations showed modest efficacy but less potency compared to PDE5 inhibitors and substantial side effects (nausea, hypotension) limit its role.
Selected Clinical Scenarios
ED in Patients with Cardiovascular Disease
- PDE5 inhibitors are beneficial but require caution: co-prescription of nitrates is contraindicated.
- Evaluate cardiac status thoroughly; ED may be an early cardiovascular risk indicator.
- Tadalafil daily or lower doses may assist men with both ED and BPH (improving lower urinary tract symptoms).
Post-Prostatectomy ED
Nerve-sparing radical prostatectomy can preserve erectile function, but many men still develop ED due to cavernous nerve damage. Early PDE5 inhibitor use (penile rehabilitation) may aid in recovery. Intracavernosal injections or vacuum devices can be adjunctive.
Diabetic ED
Men with diabetes often exhibit microvascular and neuropathic impacts on erectile mechanisms, resulting in higher PDE5 failure rates. Aggressive glycemic control, PDE5 inhibitor dose optimization, and second-line therapies (intracavernosal injections) may be needed.
Psychogenic ED
Psychotherapy or counseling can help address underlying relationship or psychological stressors. PDE5 inhibitors can break the cycle of anxiety-related performance issues. Combination with sex therapy yields enhanced outcomes.
Safety, Adherence, and Monitoring
Adverse Effect Profiles
- PDE5 inhibitors: Headaches, flushing, dyspepsia, nasal congestion, rarely vision or hearing changes, priapism.
- Alprostadil injections: Penile pain, urethral bleeding, hypotension rarely.
- Testosterone therapy: Erythrocytosis, fluid retention, possible exacerbation of prostate growth.
Medication Adherence
Open communication about side effects, correct usage timing (e.g., 30–60 minutes pre-sex), and realistic expectations fosters adherence. PDE5 inhibitors may initially fail if incorrectly taken (e.g., with heavy meals or insufficient sexual stimulation).
Interaction and Contraindications
Seeing a comprehensive medication list is crucial: PDE5 inhibitors interact with potent CYP3A4 inhibitors (e.g., ritonavir, some antifungals). Nitrates remain an absolute contraindication. In men with retinitis pigmentosa, caution with PDE5 inhibitors is advisable (rarely, PDE6 mutations aggravate retinal dysfunction).
Follow-Up Assessments
Regular reassessment of therapy effectiveness, dosing needs, and adverse events ensures safe, effective long-term management. For androgen therapy, repeated measurements of testosterone levels, hematocrit, and PSA (for men over 40) are standard.
Practical Clinical Guidelines
- Initial Steps: Address modifiable risk factors (quit smoking, weight management, optimize BP and glycemic control). Check medication lists for potential contributors.
- First-Line: Offer a PDE5 inhibitor unless contraindicated. Tailor agent selection to patient preference (on-demand vs. daily), co-morbidities, and side effect tolerability. Provide instructions on timing and sexual stimulation requirement.
- Evaluation of Failure: Confirm correct usage and sufficient trial (several attempts) at maximum tolerated dose before switching or adding therapy.
- Second-Line Options: Intracavernosal alprostadil injection, vacuum devices, or combined therapy. Hormone reassessment if signs of hypogonadism exist.
- Third-Line or Specialized: Penile prosthesis surgery for men unresponsive to simpler therapies or who desire a more permanent solution. Shockwave therapy or experimental approaches might be considered in some centers.
Special Populations
Older Men
Polypharmacy, frailty, or multiple comorbid conditions necessitate cautious PDE5 dosing, ensuring no interactions exist with nitrates or alpha-blockers. Address partner expectations and possible age-related changes in sexual function.
Younger Men
Psychogenic causes or lifestyle factors (smoking, alcohol, recreational drugs) are often prominent. PDE5 inhibitors may boost sexual confidence, but psychosocial therapy is equally important when anxiety or relationship stress drives ED.
Men with Spinal Cord Injuries
Reflexogenic erections may persist depending on injury level. PDE5 inhibitors or intracavernosal agents can be effective, though complete denervation or high-level lesions may require more invasive solutions.
Psychiatric Conditions
Selective serotonin reuptake inhibitors (SSRIs) cause sexual dysfunction frequently; PDE5 inhibitors can partially offset SSRI-induced anorgasmia or ED. Avoid combinations with potent serotonergic agents to mitigate rare but serious additive serotonin syndrome risk.
Summary and Outlook
Pharmacotherapy for erectile dysfunction has transformed in the past two decades, with PDE5 inhibitors emerging as the first-line standard for most etiologies of ED. Their mechanism leveraging the NO/cGMP pathway has proven safe and effective across a wide demographic, provided no contraindications. When PDE5 inhibition alone is inadequate or contraindicated, second-line treatments—like intracavernosal alprostadil or vacuum erection devices—offer alternatives. Testosterone replacement in men with confirmed hypogonadism provides synergistic benefits, enhancing libido and PDE5 inhibitor responsiveness. Ongoing research into CGRP modulators, melanocortin agonists, and advanced regenerative therapies (shockwave, gene therapy) may yield new breakthroughs for refractory ED.
Ultimately, optimal ED treatment demands a holistic approach: addressing underlying cardiovascular and metabolic risk factors, considering psychological aspects, and engaging patients and their partners in shared decision-making. With continuing advances in pharmacology and technology, the prospects for restoring healthy sexual function to men with ED remain increasingly promising.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition
- Katzung BG, Basic & Clinical Pharmacology, 15th Edition
- Rang HP, Dale MM, Rang & Dale’s Pharmacology, 8th Edition
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.