
Introduction
Among the oldest and most widely used agents for hyperthyroidism, thionamides (alternatively “thioureas”) remain essential in patient care. These medications include propylthiouracil (PTU), methimazole, and carbimazole, commonly referred to as antithyroid or thyroid-inhibiting drugs (Goodman & Gilman, 2018). Their core mechanism involves inhibiting the synthesis of thyroid hormones, thus reducing circulating levels of T3 (triiodothyronine) and T4 (thyroxine). Whether prescribed to stabilize newly diagnosed Graves’ disease, manage toxic nodular goiter, or prepare patients for thyroidectomy or radioactive iodine (RAI) therapy, thionamides play a major role in controlling excess thyroid hormone production.
Despite a longstanding history of efficacy, thionamides present notable adverse risk profiles, especially within certain patient demographics. Careful monitoring of hematologic, hepatic, and thyroid function is imperative to navigate potentially severe outcomes, such as agranulocytosis or hepatotoxicity. Clinicians must appreciate the nuances of each drug’s pharmacology, optimal dosing strategies, side effect prevalence, and usage in contexts like pregnancy. This article offers an extensive overview of thionamide pharmacology—encompassing chemical distinctions, mechanisms of action, pharmacokinetics, clinical indications, adverse effects, and modern evidence-based practice considerations. Drawing on canonical references (Goodman & Gilman, 2018; Katzung, 2020; Rang & Dale, 2019), it serves as a comprehensive guide for physicians, pharmacists, and other healthcare providers addressing hyperthyroid conditions.
Overview of Thionamides
Chemical Background
Thionamides, derivatives of the thiourea class, contain a sulfur-linked amide that mediates critical binding to and inhibition of thyroid-peroxidase (TPO) enzyme activity. Three key agents dominate clinical use:
- Propylthiouracil (PTU): A thiouracil derivative featuring added benefits in inhibiting peripheral T4 to T3 conversion.
- Methimazole: An imidazole derivative widely favored for its potent inhibition of TPO, longer half-life, and once-daily dosing potential.
- Carbimazole: A prodrug swiftly converted to methimazole in vivo, especially in regions like Europe, Australia, and parts of Asia (Katzung, 2020).
Historical Development
Starting in the 1940s, PTU entered clinical practice, delivering a more conservative alternative to radical thyroid surgery or RAI ablation. Methimazole followed, eventually becoming the preferred agent in many countries due to its superior potency and more convenient dosing frequency. Over time, the concept of a “block and replace” or “titration” regimen emerged, bridging the idea of controlling thyroid hormone levels while mitigating hypothyroidism caused by overzealous TPO inhibition (Rang & Dale, 2019).
Mechanisms of Action
Inhibition of Thyroid Peroxidase (TPO)
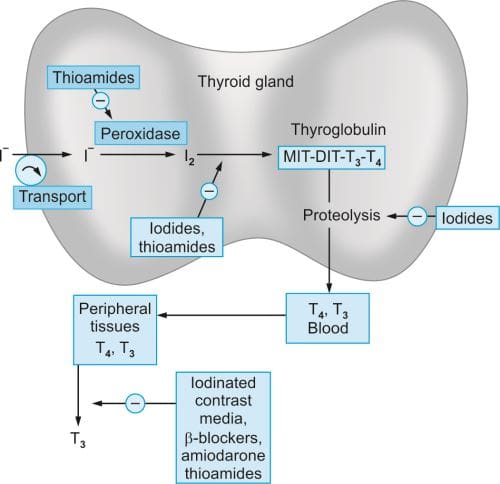
All thionamides primarily suppress TPO-mediated steps in thyroid hormone synthesis:
- Iodide Oxidation: Conversion of iodide (I⁻) to iodine (I₂).
- Iodination: Binding of activated iodide to tyrosyl residues on thyroglobulin (organification).
- Coupling: Linkage of iodotyrosine (MIT, DIT) molecules to form T3/T4 (Goodman & Gilman, 2018).
By interfering with these processes, thionamides curtail T3 and T4 production, eventually depleting stored hormone in the thyroid gland.
Inhibition of Peripheral T4–T3 Conversion
Propylthiouracil uniquely impedes the peripheral monodeiodination of T4 to T3 by inhibiting the enzyme 5′-deiodinase. While this property can be advantageous in severe thyrotoxicosis (like thyroid storm), it can also shape drug selection for particular patient subsets. Notably, methimazole and carbimazole lack this robust blockade of T4 to T3 conversion (Katzung, 2020).
Net Effects
Through TPO suppression, thionamides reduce further hormone synthesis and, via PTU’s additional benefit, can decrease T3 generation systemically. This leads to a progressive decline in circulating thyroid hormone levels and alleviation of hyperthyroid symptoms.
Pharmacokinetics
Absorption
- Methimazole: Rapidly absorbed via the GI tract, peaking in plasma around 1–2 hours post ingestion. Absorption can approximate 90–100%.
- Propylthiouracil: Absorption is variable (~50–80%), with peak levels in 1 hour.
- Carbimazole: Quickly metabolized to methimazole within the body, conferring near-equivalent kinetics to methimazole eventually (Rang & Dale, 2019).
Distribution and Protein Binding
- Methimazole: Minimal protein binding; distributed widely throughout tissues, crossing the placental barrier and secreted into breast milk at moderate levels.
- PTU: Profound protein binding (>70%), limiting transplacental passage somewhat compared to methimazole (Katzung, 2020).
Metabolism
- Methimazole undergoes hepatic metabolism to inactive compounds.
- PTU is also metabolized largely in the liver, but with shorter half-life (~1–2 hours) compared to methimazole (~6–9 hours).
- Carbimazole is structurally transformed to methimazole, retaining a half-life akin to methimazole’s profile.
Excretion
Renal excretion of metabolites (including partially unchanged drug) is the principal elimination route. Reduced kidney function can moderately prolong clearance, although dose adjustments are not always strictly mandatory (Goodman & Gilman, 2018).
Clinical Implications
- Dosing Frequency: Methimazole’s extended half-life allows once or twice-daily regimens, boosting adherence. PTU, with shorter half-life, typically warrants 2–3 daily doses.
- Onset of Action: Owing to pre-existing hormone stores in the thyroid gland, tangible clinical improvement can lag by several weeks, irrespective of the thionamide used (Katzung, 2020).
Clinical Uses
Graves’ Disease
Graves’ disease, an autoimmune cause of hyperthyroidism, stands as the most frequent indication for thionamides. Patients may receive:
- Titration Regimen: Gradually adjusting the thionamide dose to normalize thyroid function.
- Block-and-Replace Regimen: Higher doses to fully suppress thyroid hormone production, concurrently giving levothyroxine to maintain normal T4/T3 levels (Rang & Dale, 2019).
Pretreatment Before Thyroidectomy
Short-duration (weeks to months) of methimazole or PTU can shrink the hyperactive gland, reduce vascularity, and stabilize the patient’s metabolic state prior to surgery. Additionally, concurrent iodine solutions (e.g., Lugol’s iodine) further decrease vascularization for easier surgical resection (Katzung, 2020).
Preparation for Radioactive Iodine (RAI)
In certain protocols, thionamides help achieve euthyroidism prior to RAI therapy, minimizing post-RAI thyroid hormone surges. Some providers pause methimazole or PTU before RAI to maximize the radioisotope’s effectiveness, then restart after a brief interval if needed (Goodman & Gilman, 2018).
Thyroid Storm
In life-threatening thyroid storm, PTU is often favored initially for its dual suppression (both hormone synthesis and peripheral T3 production). Combination treatment with beta-blockers, corticosteroids, and supportive measures is standard (Rang & Dale, 2019).
Toxic Nodular Goiter
Patients with single or multinodular toxic adenomas can benefit from methimazole or carbimazole to control hormone excess, either as bridging therapy ahead of surgery or if they are poor surgical candidates (Katzung, 2020).
Dosage and Administration
Methimazole
- Initial Adult Dose: 10–30 mg daily (mild to moderate hyperthyroidism); up to ~40 mg in severe cases.
- Maintenance: 5–10 mg daily.
- Once-Daily Dosing: Feasible due to longer half-life.
Propylthiouracil
- Initial Adult Dose: 50–150 mg three times daily (total daily 150–450 mg) for moderate hyperthyroidism; possibly higher in severe scenarios.
- Maintenance: ~50 mg two or three times daily as euthyroidism is achieved (Goodman & Gilman, 2018).
Carbimazole
- Typically 20–60 mg/day in divided doses: once converted to methimazole, ~40 mg of carbimazole ~ 26 mg methimazole activity. Maintenance around 5–15 mg/day.
Individualizing Regimens
- Severity of Hyperthyroidism: Higher initial doses for very high T3/T4 levels.
- Patient Factors: Age, weight, comorbidities, pregnancy status, compliance potential.
- Monitoring: TSH, Free T4, clinical signs every 4–6 weeks initially to adjust dosing (Katzung, 2020).
Adverse Effects and Toxicities
Agranulocytosis
A rare but grave complication (0.2–0.5%), agranulocytosis can present with fever, oropharyngeal infection, and sudden drop in neutrophils. It requires immediate drug discontinuation plus supportive therapy (e.g., granulocyte colony-stimulating factor). All patients should be counseled to halt medication and seek care if they develop a severe sore throat or fever (Rang & Dale, 2019).
Hepatotoxicity
- PTU can cause severe hepatic injury, including fulminant liver failure, albeit rarely. This risk is greater than that with methimazole.
- Methimazole typically yields a milder cholestatic picture if hepatic involvement arises (Goodman & Gilman, 2018).
Rash and Allergy
Approximately 5% experience maculopapular rash, pruritus, or urticaria. Some can tolerate alternative agents (e.g., switching from PTU to methimazole) if the rash is mild and non-cross-reactive. Severe vasculitis or SLE-like syndromes are rarer but recognized (Katzung, 2020).
Others
• Arthralgias
• Gastrointestinal upset
• Reduced taste sensation (dysgeusia) or abnormal smell perceptionIn certain patients, indefinite therapy may be infeasible if side effects are intolerable.
Thionamides in Pregnancy
Teratogenicity Concerns
- Methimazole is associated (rarely) with aplasia cutis (absence of a portion of skin), and rare but serious embryopathies.
- PTU has lower risk of embryopathy but higher potential for severe hepatotoxicity in the mother (Katzung, 2020).
Clinical Recommendations
During the first trimester, many guidelines favor PTU in small to moderate doses to minimize methimazole teratogenic risk. After the first trimester, switching to methimazole is often recommended to avoid PTU-related hepatotoxicity (Rang & Dale, 2019). Nonetheless, controversies persist; treatment must be individualized.
Breastfeeding
Both methimazole and PTU appear in breast milk, but in modest amounts. Methimazole is commonly deemed acceptable at minimal effective doses. Monitoring infant thyroid function is prudent (Goodman & Gilman, 2018).
Comparisons and Contrasts

Methimazole vs. Propylthiouracil
- Potency and Half-life: Methimazole is ~10 times more potent and has an extended half-life, easing dosing frequency. PTU requires multiple daily dosing.
- Peripheral T3 Block: Only PTU significantly inhibits peripheral T4–T3 conversion.
- Adverse Profile: PTU → greater hepatic toxicity risk, often reserved for pregnancy first trimester or thyroid storm. Methimazole → more common usage overall, with easier compliance (Katzung, 2020).
Carbimazole vs. Methimazole
Carbimazole is a prodrug swiftly converted to methimazole in vivo, sharing the latter’s profile. The choice between them often hinges on regional availability or physician preference (Rang & Dale, 2019).
Beta-Blockers & Adjuncts
While not directly part of thionamide therapy, beta-blockers (e.g., propranolol) frequently combine with methimazole or PTU to attenuate sympathetic-driven hyperthyroid manifestations (tachycardia, tremor). Additionally, iodides or radioiodine therapy might accompany or follow thionamide usage, depending on the treatment algorithm (Goodman & Gilman, 2018).
Resistance and Treatment Failure
True Resistance
Rare for TPO to mutate significantly and become fully unresponsive to thionamides. Treatment “failure” frequently reflects nonadherence, inadequate dosing, or extreme disease severity (Katzung, 2020).
Strategies if Suboptimal Response
- Reassess compliance, check TSH and T3/T4 frequently.
- Evaluate for interfering medications or malabsorption.
- Optimize dosage or switch from PTU to methimazole (or vice versa) if side effects hamper therapy.
- Consider alternate definitive interventions (radioiodine or surgery) when medical management is insufficient or not tolerated (Rang & Dale, 2019).
Monitoring Therapy
Biochemical Markers
- Free T4 (FT4) and Total T3: Reflect current hormone production; typically monitored every 4–6 weeks initially.
- TSH: Often lags behind changes in T3/T4; can remain suppressed for weeks after hormone normalization.
- Clinical Symptoms: Tachycardia resolution, weight gain, improved tremor, reduced anxiety are indicators of better control (Goodman & Gilman, 2018).
Treatment Duration
Commonly, 12–18 months of therapy, then medication weaning is trialed. About 40–50% of Graves’ disease patients may achieve remission. However, relapse can occur—if so, permanent solutions (RAI or surgery) might be considered (Katzung, 2020).
Special Clinical Scenarios
Thyroid Storm
An acute, life-threatening exacerbation of hyperthyroidism demands:
- High-dose PTU to block new thyroid hormone synthesis + peripheral T3 generation.
- Beta-blockade (propranolol or esmolol).
- Corticosteroids (hydrocortisone) to inhibit T4–T3 conversion and address potential relative adrenal insufficiency.
- Supportive measures: Cooling, IV fluids, sedation (Rang & Dale, 2019).
Neonatal Hyperthyroidism
When maternal Graves’ disease includes transplacental TSH receptor-stimulating antibodies, neonates can present with hyperthyroidism. Methimazole is often given in tiny doses to control the infant’s condition. Monitoring is paramount (Goodman & Gilman, 2018).
Subclinical Hyperthyroidism
Persistently low TSH with normal T3/T4 sometimes prompts mild-dose methimazole or watchful waiting, especially in older adults with arrhythmia risks or osteoporosis risk factors. The approach is individualized based on symptom burden and potential for disease progression (Katzung, 2020).
Concomitant Illnesses
Patients with hepatic dysfunction or prior agranulocytosis demand heightened caution. PTU usage might be restricted in those with existing liver disease, while methimazole’s potential for cholestatic injury must also be kept in mind. Blood cell counts are needed per any suggestion of infection or unusual fatigue (Rang & Dale, 2019).
Adherence and Patient Counseling
Side Effect Recognition
Patients must be educated on early signs of adverse reactions such as:
- Sore throat, fever → possible agranulocytosis.
- Jaundice, malaise → potential liver toxicity.
- Rash → consider alternative therapy.
Immediate reporting and cessation of the drug pending further evaluation can prevent severe complications (Goodman & Gilman, 2018).
Importance of Monitoring
Regular check-ups (lab assessments every 4–8 weeks) remain critical. Nonadherence can prompt abrupt hormone relapses or partial therapy resulting in suboptimal disease control.
Lifestyle Factors
Adequate rest, stress reduction, and consistent follow-up with endocrinology can further optimize hyperthyroid management. If surgery or RAI becomes necessary, bridging with thionamides ensures safer outcomes (Katzung, 2020).
Thionamides and Modern Practice
Shifting Preferences
Given the safety profile, methimazole has emerged as the first-line agent except in specific exceptions:
- First Trimester of Pregnancy: PTU is preferred due to reduced teratogenic risk, despite higher hepatotoxicity concerns.
- Acute Thyroid Storm: PTU’s additional peripheral T4–T3 block is beneficial in severe crises (Rang & Dale, 2019).
Outside these contexts, methimazole’s once-daily regimen and fewer serious hepatic adverse events make it generally favored.
Debates around Definitive Therapy
In multi-ethnic or resource-variable settings, indefinite methimazole or PTU therapy can manage hyperthyroidism, though many patients prefer definitive cures (radioiodine or surgery). Patient education, cost considerations, and risk–benefit analyses shape decisions (Goodman & Gilman, 2018).
Evolving Research
Recent studies explore whether lower-dose methimazole regimens can effectively maintain remission, potentially lowering the incidence of side effects. Genetic factors influencing TPO or deiodinase enzymes could tailor individualized therapy in the future. The phenomenon of “immunological remission” through extended thionamide therapy (modulating T-lymphocyte function) is another intriguing dimension (Katzung, 2020).
Limitations and Key Points
- Narrow Therapeutic Window: Thionamides often have significant adverse outcomes (hepatotoxicity, agranulocytosis) requiring vigilance.
- Delayed Onset: Clinical improvement typically appears several weeks after starting therapy due to stored thyroid hormone depletion.
- Relapse: Many patients eventually relapse post-thionamide withdrawal, indicating possible need for second-line interventions.
- Special Situations: Unique strategies or drug preferences exist in pregnancy, thyroid storm, and hepatic compromise (Rang & Dale, 2019).
Future Perspectives
Personalized Thyroid Pharmacotherapy
Ongoing research delves into pharmacogenomics—exploring polymorphisms in genes controlling drug metabolism (CYP enzymes, NAT2), TPO variants, or immune pathways leading to differential responses. Identifying biomarkers for sustained remission might reduce undue exposure or hasten definitive therapy recommendations (Goodman & Gilman, 2018).
Novel Anti-Thyroid Agents
While no immediate successors to thionamides appear imminent, potential compounds modulating TSH receptor or advanced TPO inhibitors could eventually enter the market. Trials must balance efficacy with minimal risk of agranulocytosis or major organ toxicity (Katzung, 2020).
Biologic Modulators
As knowledge of Graves’ disease pathogenesis grows, immunomodulators (e.g., anti-CD20 agents like rituximab) or TSH receptor-blocking antibodies might synergize or replace thionamides in refractory cases. However, cost and safety hurdles remain substantial.
Conclusion
Thionamides—chiefly methimazole, propylthiouracil (PTU), and carbimazole—occupy an essential niche in hyperthyroidism management. Their fundamental mechanism of action involves inhibition of thyroid peroxidase-mediated hormone synthesis, supplemented by PTU’s unique blockade of peripheral T4–T3 conversion (Goodman & Gilman, 2018). Widely used for conditions such as Graves’ disease, toxic nodules, and as a bridge to surgery or radioactive iodine therapy, these agents reliably restore euthyroidism over weeks to months.
In modern practice, methimazole is typically first-line, favored for once-daily dosing and lower hepatotoxic risk relative to PTU. However, PTU persists in special scenarios, such as severe thyroid storm or early pregnancy, capitalizing on its peripheral T3 blockade and possibly reduced teratogenicity. Key hazards like agranulocytosis and hepatotoxicity require vigilant monitoring—patients must be aware of early signs of infection or jaundice. Despite a substantial relapse rate after therapy cessation, thionamides can induce sustained immunological remission in some cohorts, averting the need for radical interventions (Katzung, 2020).
As research continues elucidating immunogenetic underpinnings, improvements in personalized hyperthyroid treatment regimens may evolve—potentially refining current cycles of “treat and see” to minimize adverse events, optimize remission, and integrate advanced immunologic or biologic therapies. Until then, thionamides remain a cornerstone in the dynamic landscape of hyperthyroid management, anchoring a decades-long clinical legacy while shaping tomorrow’s best practices (Rang & Dale, 2019).
References (Book Citations)
Rang HP, Dale MM, Rang & Dale’s Pharmacology, 8th Edition.
Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition.
Katzung BG, Basic & Clinical Pharmacology, 14th Edition.
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.