

1 · Introduction
Vomiting (emesis) is an evolutionarily conserved defence reflex that forcefully expels gastric—and at times intestinal—contents through the mouth. Although the motor act seems singular, it is orchestrated by a distributed brain-stem network that integrates sensory danger signals from the gut, the bloodstream, the vestibular system and higher cortical areas. Two functional loci dominate classical descriptions:
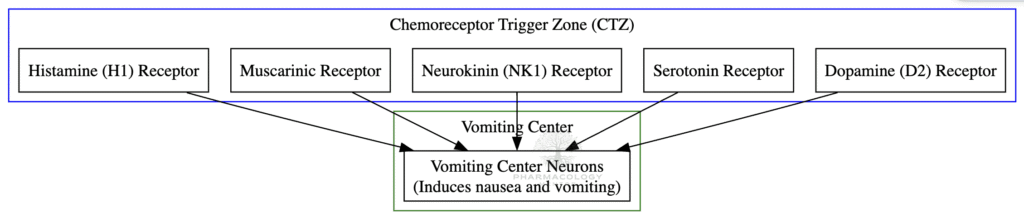
- The “vomiting centre” (VC)—a loosely delimited collection of medullary nuclei that integrates emetic inputs and produces the patterned motor output.
- The chemoreceptor trigger zone (CTZ)—a specialised sensory circumventricular organ located in the area postrema that samples blood and cerebrospinal fluid (CSF) for circulating emetogens and relays this information to the VC.
A clear grasp of their anatomy, neurochemistry and physiology underpins modern anti-emetic pharmacology used in chemotherapy, postoperative care, motion sickness and numerous systemic diseases.
2 · Historical Perspective
Systematic study of emesis began in the late nineteenth century when physiologists noted that sectioning the vagus did not always abolish vomiting, hinting at a central driver. In the 1950s, Borison and Wang produced the first detailed mapping of the dorsal medulla in cats, distinguishing a “vomiting centre” from the adjacent area postrema. Subsequent lesion and micro-injection studies confirmed that:
- Destruction of the area postrema abolishes emesis triggered by blood-borne agents but not by vagal stimulation.
- Focal chemical excitation of the nucleus tractus solitarius (NTS) or nearby reticular formation elicits the full behavioural pattern of vomiting.
The term chemoreceptor trigger zone (CTZ) was formally coined in the 1960s; by the 1990s, c-Fos immunohistochemistry and neuro-tracing had further clarified afferent–efferent circuitry. What began as crude localisation has matured into a sophisticated receptor-level map that guides today’s targeted anti-emetic drug design.
3 · Macro-anatomy
3.1 The Vomiting Centre (VC)
The VC is not a discrete nucleus but a network extending through the dorsolateral medulla and lower pons. Principal components include:
- Nucleus tractus solitarius (NTS)—the major visceral sensory nucleus receiving vagal, glossopharyngeal and spinal visceral afferents.
- Dorsal motor nucleus of the vagus (DMV)—parasympathetic output to upper GI tract.
- Nucleus ambiguus & reticular formation—premotor elements that coordinate pharyngeal, laryngeal, respiratory and abdominal muscles.
- Adjacent respiratory pattern generators—ensuring airway protection and timing respiratory arrest during emesis.
3.2 The Area Postrema and CTZ
The CTZ resides in the area postrema, a paired, tongue-shaped structure on the caudal floor of the fourth ventricle just rostral to the obex. Key anatomic features:
- Lack of a blood–brain barrier—fenestrated capillaries and sparse tight junctions expose neurons to circulating molecules.
- Slow blood flow—prolongs contact time for toxin detection.
- Intimate connections—dense reciprocal projections with the NTS form a dorsal vagal complex that acts as a single chemosensory hub.
4 · Cellular Neurochemistry
Multiple neurotransmitters and receptors coexist in the CTZ and VC. Their differential distribution explains why clinically distinct classes of anti-emetics can be combined additively (Table 1).
| Receptor | Dominant Location | Afferent Agonists | Therapeutic Antagonists |
|---|---|---|---|
| 5-HT3 | CTZ, NTS, vagal afferents | Cisplatin, radiation-induced 5-HT | Ondansetron, Palonosetron |
| D2 | CTZ ≫ VC | Apomorphine, low-dose opioids | Metoclopramide, Domperidone |
| NK1 | CTZ, NTS | Substance P, stress peptides | Aprepitant, Fosaprepitant |
| H1 | Vestibular nuclei, CTZ | Histamine (motion) | Promethazine, Meclizine |
| M1 | Vestibular nuclei | Muscarinic agonists | Scopolamine |
Table 1 — Major receptor systems relevant to emesis and their pharmacological antagonists.
Other modulators include GABA, endogenous cannabinoids, enkephalins and cAMP-linked PDE-4 mechanisms. It is the co-activation of receptor populations that ultimately decides whether the VC threshold for motor pattern generation is reached.
5 · Physiology of the Emetic Reflex

5.1 Afferent Inputs
- Humoral route—blood-borne toxins, drugs and metabolic derangements activate CTZ receptors directly.
- Visceral/vagal route—irritation of gut mucosa triggers enterochromaffin 5-HT release, stimulating 5-HT3-bearing vagal afferents that terminate in the NTS.
- Vestibular route—motion generates mismatch signals processed by vestibular nuclei rich in H1/M1 receptors.
- Cortico-limbic route—odours, memories or emotional distress reach the VC via the insula, amygdala and hypothalamus.
5.2 Central Pattern Generation
All afferents converge on the NTS, which in turn drives a central pattern generator (CPG) within the reticular formation. The CPG imposes a stereotyped temporal sequence:
- Prodromal autonomic surge—salivation, pallor, tachycardia.
- Retching—rhythmic contractions of abdominal musculature against a closed glottis.
- Expulsion—simultaneous diaphragm descent, abdominal wall contraction, relaxation of lower oesophageal sphincter (LOS) and rapid opening of the UOS, ejecting gastric contents.
6 · Pharmacology of Antiemetic Therapy
6.1 5-HT3 Antagonists
Ondansetron, granisetron and the long-acting palonosetron competitively block 5-HT3 receptors on vagal afferents and CTZ neurons. Palonosetron’s high receptor affinity and two-day half-life afford superior control of delayed chemotherapy-induced emesis.
6.2 D2 Antagonists
Metoclopramide provides dual benefit: central D2 blockade and peripheral pro-kinetic 5-HT4 agonism. Domperidone is largely restricted to the CTZ because it poorly crosses the intact blood–brain barrier, reducing extrapyramidal risk.
6.3 NK1 Antagonists
Aprepitant, fosaprepitant and newer agents (e.g., netupitant) prevent substance P binding at NK1 receptors in both CTZ and NTS. They synergise with 5-HT3 antagonists and dexamethasone to form standard “triple therapy” for highly emetogenic chemotherapy.
6.4 H1 / M1 Antagonists
Promethazine, meclizine and dimenhydrinate (H1) or transdermal scopolamine (M1) are the mainstay for motion sickness, reflecting the vestibular bias of these receptors.
6.5 Adjunctive Agents
- Corticosteroids—dexamethasone may inhibit prostaglandin synthesis within the NTS.
- Atypical antipsychotics—low-dose olanzapine offers broad-spectrum receptor blockade for refractory nausea.
- Cannabinoids—dronabinol and nabilone activate CB1 receptors in the NTS, though psychotropic effects limit routine use.
7 · Pathophysiology in Clinical Context
7.1 Chemotherapy-Induced Nausea & Vomiting (CINV)
Cytotoxic drugs such as cisplatin provoke massive 5-HT release from enterochromaffin cells within hours (acute phase), followed 24–72 h later by substance P-mediated activation of NK1 receptors (delayed phase). Triple therapy has reduced emesis rates from >90% to under 10% in modern protocols.
7.2 Post-Operative Nausea & Vomiting (PONV)
Volatile anaesthetics, nitrous oxide and intra-operative opioids stimulate CTZ D2 and μ-opioid receptors. Female sex, non-smoking status and prior motion sickness magnify susceptibility. Risk-stratified prophylaxis employs 5-HT3 antagonists ± dexamethasone; high-risk cases receive NK1 blockade.
7.3 Opioid Pharmacodynamics
Intriguingly, opioids are bi-phasic: low doses access the CTZ (outside the BBB) and trigger emesis; higher sustained concentrations penetrate the BBB, activating μ-receptors in the NTS and cortex that dampen the reflex. Clinically, a patient may vomit after the first dose but tolerate subsequent doses.
7.4 Pregnancy-Related Emesis
Rising human chorionic gonadotropin (hCG) and oestrogen sensitize CTZ 5-HT3/D2 pathways in early gestation. First-line therapy uses vitamin B6 with doxylamine; severe hyperemesis gravidarum may require ondansetron or metoclopramide after careful risk assessment.
7.5 Motion Sickness
Visual–vestibular mismatch activates cholinergic vestibular projections to the VC. Prophylaxis with scopolamine patches or sedating antihistamines remains the gold standard for long voyages or aviation.
7.6 Area Postrema Syndromes
In neuromyelitis optica spectrum disorder (NMOSD), auto-antibodies against aquaporin-4 preferentially inflame the area postrema, producing intractable hiccups, nausea and vomiting—often preceding optic nerve or spinal cord attacks by months.
8 · Emerging & Experimental Insights
- PDE-4 inhibitors—agents like rolipram elevate cAMP in CTZ neurons and are profoundly emetogenic, limiting their systemic use as anti-inflammatories.
- HCN channel modulators—hyperpolarisation-activated cyclic nucleotide (HCN) channels modulate CTZ neuronal pacemaker activity; blockade attenuates conditioned taste aversion in rodents.
- Gut–brain peptides—GLP-1 receptor agonists improving glycaemic control frequently provoke nausea via CTZ activation; “biased” agonists seeking metabolic benefit without emesis are in development.
9 · Integration with Autonomic & Respiratory Control
During emesis, diaphragmatic descent and abdominal compression raise intra-gastric and intra-thoracic pressures dramatically. Respiratory CPGs coordinate a brief apnoea and glottic closure to protect the airway, while cardiovascular nuclei in the medulla mediate a vagal bradycardia and vasodepressor response that many patients experience as presyncope.
10 · Practical Bedside Correlations
- Apomorphine test—a potent D2 agonist, once used in Parkinson’s disease, induces vomiting within minutes; its emetic liability demands pre-treatment with ondansetron or domperidone.
- Syrup of ipecac—acts peripherally on gastric mucosa and centrally on the CTZ; obsolete for poisoning because of poor efficacy and cardiac toxicity.
- Projectile vomiting in posterior fossa tumours—raised intracranial pressure or direct compression of the VC causes sudden, unprovoked emesis often without preceding nausea.
- Radiation sickness—ionising radiation injures intestinal mucosa, releasing 5-HT; 5-HT3 antagonists form the cornerstone of prophylaxis during ablative radiotherapy.
11 · Key Learning Points
- CTZ = sensor, VC = integrator/effector.
- Distinct receptor topography underlies selective anti-emetic drug classes.
- CINV, PONV and motion sickness differ in dominant afferent pathways and therefore in optimal prophylaxis.
- Opioids exhibit dose-dependent emetic and anti-emetic effects owing to differential blood–brain barrier penetration.
- Area postrema lesions may herald autoimmune brain-stem disease such as NMOSD.
12 · Conclusion
The intertwined vomiting centre and chemoreceptor trigger zone embody the elegance of brain–gut integration. From primordial protection against ingested toxins to contemporary challenges posed by cytotoxic chemotherapy, these structures detect danger, compute threat and execute a life-preserving expulsion reflex with remarkable precision. Advances in receptor pharmacology, neuro-immune understanding and gut peptide signalling are ushering in ever more selective anti-emetic therapies, promising relief to patients across oncology, surgery, obstetrics and beyond.
Medical Disclaimer
The medical information on this post is for general educational purposes only and is provided by Pharmacology Mentor. While we strive to keep content current and accurate, Pharmacology Mentor makes no representations or warranties, express or implied, regarding the completeness, accuracy, reliability, suitability, or availability of the post, the website, or any information, products, services, or related graphics for any purpose. This content is not a substitute for professional medical advice, diagnosis, or treatment; always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition and never disregard or delay seeking professional advice because of something you have read here. Reliance on any information provided is solely at your own risk.